Mina Stephanos, Christopher M B Stewart, Ameen Mahmood, Christopher Brown, Shahin Hajibandeh, Shahab Hajibandeh, Thomas Satyadas
{"title":"腹腔镜肝脏切除术中低中心静脉压与标准中心静脉压的比较:系统综述、荟萃分析和试验序列分析。","authors":"Mina Stephanos, Christopher M B Stewart, Ameen Mahmood, Christopher Brown, Shahin Hajibandeh, Shahab Hajibandeh, Thomas Satyadas","doi":"10.14701/ahbps.23-137","DOIUrl":null,"url":null,"abstract":"<p><p>To compare the outcomes of low central venous pressure (CVP) to standard CVP during laparoscopic liver resection. The study design was a systematic review following the PRISMA statement standards. The available literature was searched to identify all studies comparing low CVP with standard CVP in patients undergoing laparoscopic liver resection. The outcomes included intraoperative blood loss (primary outcome), need for blood transfusion, mean arterial pressure, operative time, Pringle time, and total complications. Random- effects modelling was applied for analyses. Type I and type II errors were assessed by trial sequential analysis (TSA). A total of 8 studies including 682 patients were included (low CVP group, 342; standard CVP group, 340). Low CVP reduced intraoperative blood loss during laparoscopic liver resection (mean difference [MD], -193.49 mL; 95% confidence interval [CI], -339.86 to -47.12; <i>p</i> = 0.01). However, low CVP did not have any effect on blood transfusion requirement (odds ratio [OR], 0.54; 95% CI, 0.28-1.03; <i>p</i> = 0.06), mean arterial pressure (MD, -1.55 mm Hg; 95% CI, -3.85-0.75; <i>p</i> = 0.19), Pringle time (MD, -0.99 minutes; 95% CI, -5.82-3.84; <i>p</i> = 0.69), operative time (MD, -16.38 minutes; 95% CI, -36.68-3.39; <i>p</i> = 0.11), or total complications (OR, 1.92; 95% CI, 0.97-3.80; <i>p</i> = 0.06). TSA suggested that the meta-analysis for the primary outcome was not subject to type I or II errors. Low CVP may reduce intraoperative blood loss during laparoscopic liver resection (moderate certainty); however, this may not translate into shorter operative time, shorter Pringle time, or less need for blood transfusion. Randomized controlled trials with larger sample sizes will provide more robust evidence.</p>","PeriodicalId":72220,"journal":{"name":"Annals of hepato-biliary-pancreatic surgery","volume":" ","pages":"115-124"},"PeriodicalIF":1.7000,"publicationDate":"2024-05-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11128796/pdf/","citationCount":"0","resultStr":"{\"title\":\"Low versus standard central venous pressure during laparoscopic liver resection: A systematic review, meta-analysis and trial sequential analysis.\",\"authors\":\"Mina Stephanos, Christopher M B Stewart, Ameen Mahmood, Christopher Brown, Shahin Hajibandeh, Shahab Hajibandeh, Thomas Satyadas\",\"doi\":\"10.14701/ahbps.23-137\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>To compare the outcomes of low central venous pressure (CVP) to standard CVP during laparoscopic liver resection. The study design was a systematic review following the PRISMA statement standards. The available literature was searched to identify all studies comparing low CVP with standard CVP in patients undergoing laparoscopic liver resection. The outcomes included intraoperative blood loss (primary outcome), need for blood transfusion, mean arterial pressure, operative time, Pringle time, and total complications. Random- effects modelling was applied for analyses. Type I and type II errors were assessed by trial sequential analysis (TSA). A total of 8 studies including 682 patients were included (low CVP group, 342; standard CVP group, 340). Low CVP reduced intraoperative blood loss during laparoscopic liver resection (mean difference [MD], -193.49 mL; 95% confidence interval [CI], -339.86 to -47.12; <i>p</i> = 0.01). However, low CVP did not have any effect on blood transfusion requirement (odds ratio [OR], 0.54; 95% CI, 0.28-1.03; <i>p</i> = 0.06), mean arterial pressure (MD, -1.55 mm Hg; 95% CI, -3.85-0.75; <i>p</i> = 0.19), Pringle time (MD, -0.99 minutes; 95% CI, -5.82-3.84; <i>p</i> = 0.69), operative time (MD, -16.38 minutes; 95% CI, -36.68-3.39; <i>p</i> = 0.11), or total complications (OR, 1.92; 95% CI, 0.97-3.80; <i>p</i> = 0.06). TSA suggested that the meta-analysis for the primary outcome was not subject to type I or II errors. Low CVP may reduce intraoperative blood loss during laparoscopic liver resection (moderate certainty); however, this may not translate into shorter operative time, shorter Pringle time, or less need for blood transfusion. Randomized controlled trials with larger sample sizes will provide more robust evidence.</p>\",\"PeriodicalId\":72220,\"journal\":{\"name\":\"Annals of hepato-biliary-pancreatic surgery\",\"volume\":\" \",\"pages\":\"115-124\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2024-05-31\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11128796/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of hepato-biliary-pancreatic surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14701/ahbps.23-137\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/2/16 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of hepato-biliary-pancreatic surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14701/ahbps.23-137","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/2/16 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Low versus standard central venous pressure during laparoscopic liver resection: A systematic review, meta-analysis and trial sequential analysis.
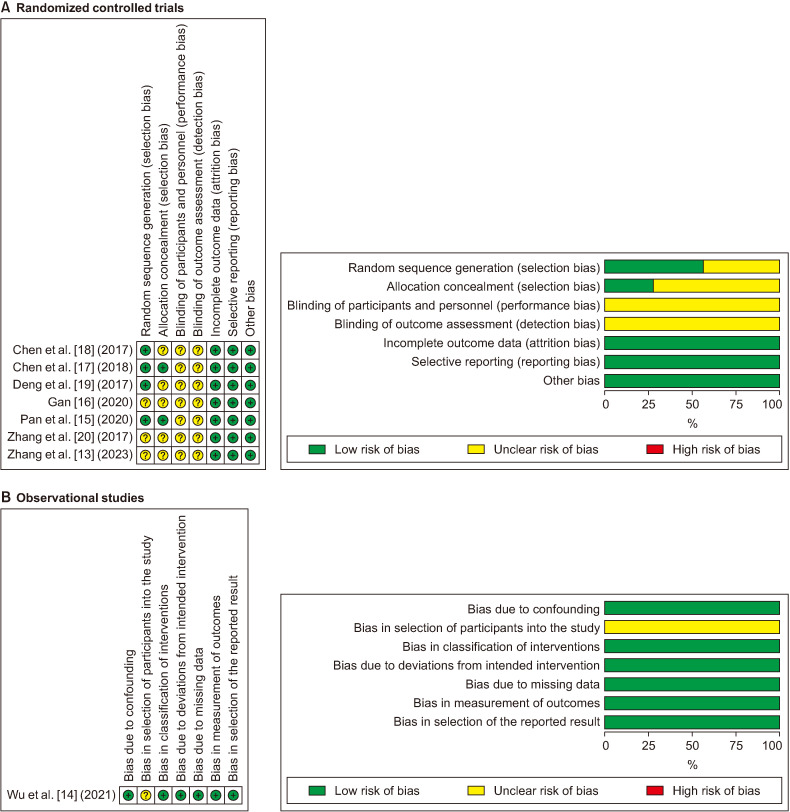
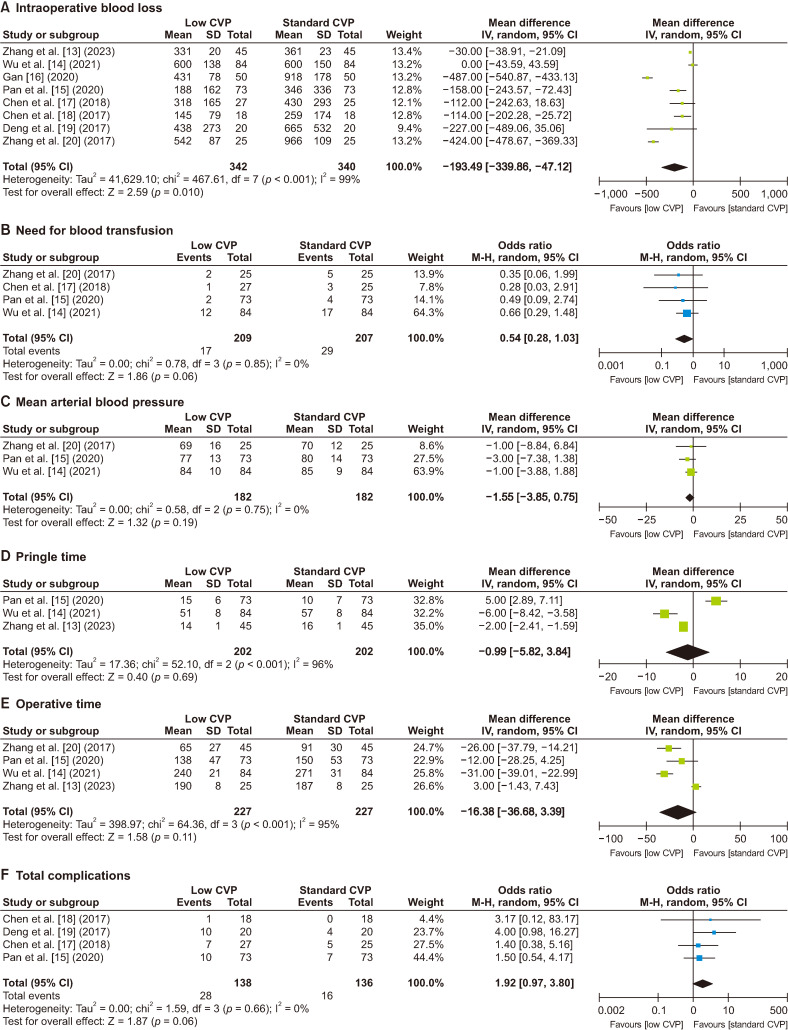
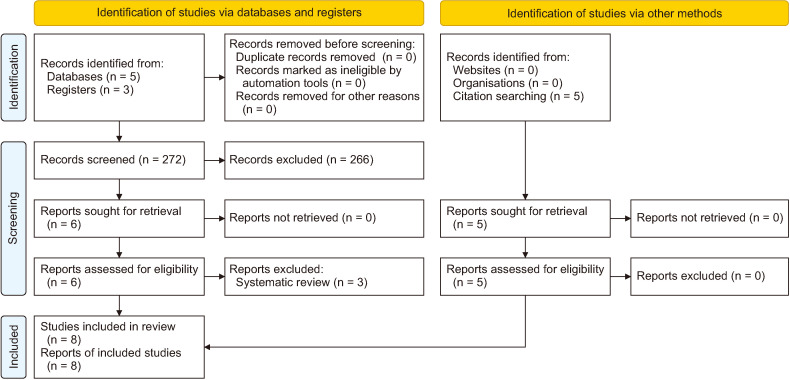
To compare the outcomes of low central venous pressure (CVP) to standard CVP during laparoscopic liver resection. The study design was a systematic review following the PRISMA statement standards. The available literature was searched to identify all studies comparing low CVP with standard CVP in patients undergoing laparoscopic liver resection. The outcomes included intraoperative blood loss (primary outcome), need for blood transfusion, mean arterial pressure, operative time, Pringle time, and total complications. Random- effects modelling was applied for analyses. Type I and type II errors were assessed by trial sequential analysis (TSA). A total of 8 studies including 682 patients were included (low CVP group, 342; standard CVP group, 340). Low CVP reduced intraoperative blood loss during laparoscopic liver resection (mean difference [MD], -193.49 mL; 95% confidence interval [CI], -339.86 to -47.12; p = 0.01). However, low CVP did not have any effect on blood transfusion requirement (odds ratio [OR], 0.54; 95% CI, 0.28-1.03; p = 0.06), mean arterial pressure (MD, -1.55 mm Hg; 95% CI, -3.85-0.75; p = 0.19), Pringle time (MD, -0.99 minutes; 95% CI, -5.82-3.84; p = 0.69), operative time (MD, -16.38 minutes; 95% CI, -36.68-3.39; p = 0.11), or total complications (OR, 1.92; 95% CI, 0.97-3.80; p = 0.06). TSA suggested that the meta-analysis for the primary outcome was not subject to type I or II errors. Low CVP may reduce intraoperative blood loss during laparoscopic liver resection (moderate certainty); however, this may not translate into shorter operative time, shorter Pringle time, or less need for blood transfusion. Randomized controlled trials with larger sample sizes will provide more robust evidence.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


