Bahadar S Bhatia, John F Morlese, Sarah Yusuf, Yiting Xie, Bob Schallhorn, David Gruen
{"title":"利用深度学习和自然语言处理胸部算法验证的阳性预测值,对放射科医生的诊断准确性进行真实世界评估。","authors":"Bahadar S Bhatia, John F Morlese, Sarah Yusuf, Yiting Xie, Bob Schallhorn, David Gruen","doi":"10.1093/bjro/tzad009","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>This diagnostic study assessed the accuracy of radiologists retrospectively, using the deep learning and natural language processing chest algorithms implemented in Clinical Review version 3.2 for: pneumothorax, rib fractures in digital chest X-ray radiographs (CXR); aortic aneurysm, pulmonary nodules, emphysema, and pulmonary embolism in CT images.</p><p><strong>Methods: </strong>The study design was double-blind (artificial intelligence [AI] algorithms and humans), retrospective, non-interventional, and at a single NHS Trust. Adult patients (≥18 years old) scheduled for CXR and CT were invited to enroll as participants through an opt-out process. Reports and images were de-identified, processed retrospectively, and AI-flagged discrepant findings were assigned to two lead radiologists, each blinded to patient identifiers and original radiologist. The radiologist's findings for each clinical condition were tallied as a verified discrepancy (true positive) or not (false positive).</p><p><strong>Results: </strong>The missed findings were: 0.02% rib fractures, 0.51% aortic aneurysm, 0.32% pulmonary nodules, 0.92% emphysema, and 0.28% pulmonary embolism. The positive predictive values (PPVs) were: pneumothorax (0%), rib fractures (5.6%), aortic dilatation (43.2%), pulmonary emphysema (46.0%), pulmonary embolus (11.5%), and pulmonary nodules (9.2%). The PPV for pneumothorax was nil owing to lack of available studies that were analysed for outpatient activity.</p><p><strong>Conclusions: </strong>The number of missed findings was far less than generally predicted. The chest algorithms deployed retrospectively were a useful quality tool and AI augmented the radiologists' workflow.</p><p><strong>Advances in knowledge: </strong>The diagnostic accuracy of our radiologists generated missed findings of 0.02% for rib fractures CXR, 0.51% for aortic dilatation, 0.32% for pulmonary nodule, 0.92% for pulmonary emphysema, and 0.28% for pulmonary embolism for CT studies, all retrospectively evaluated with AI used as a quality tool to flag potential missed findings. It is important to account for prevalence of these chest conditions in clinical context and use appropriate clinical thresholds for decision-making, not relying solely on AI.</p>","PeriodicalId":72419,"journal":{"name":"BJR open","volume":"6 1","pages":"tzad009"},"PeriodicalIF":2.1000,"publicationDate":"2023-12-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10860529/pdf/","citationCount":"0","resultStr":"{\"title\":\"A real-world evaluation of the diagnostic accuracy of radiologists using positive predictive values verified from deep learning and natural language processing chest algorithms deployed retrospectively.\",\"authors\":\"Bahadar S Bhatia, John F Morlese, Sarah Yusuf, Yiting Xie, Bob Schallhorn, David Gruen\",\"doi\":\"10.1093/bjro/tzad009\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>This diagnostic study assessed the accuracy of radiologists retrospectively, using the deep learning and natural language processing chest algorithms implemented in Clinical Review version 3.2 for: pneumothorax, rib fractures in digital chest X-ray radiographs (CXR); aortic aneurysm, pulmonary nodules, emphysema, and pulmonary embolism in CT images.</p><p><strong>Methods: </strong>The study design was double-blind (artificial intelligence [AI] algorithms and humans), retrospective, non-interventional, and at a single NHS Trust. Adult patients (≥18 years old) scheduled for CXR and CT were invited to enroll as participants through an opt-out process. Reports and images were de-identified, processed retrospectively, and AI-flagged discrepant findings were assigned to two lead radiologists, each blinded to patient identifiers and original radiologist. The radiologist's findings for each clinical condition were tallied as a verified discrepancy (true positive) or not (false positive).</p><p><strong>Results: </strong>The missed findings were: 0.02% rib fractures, 0.51% aortic aneurysm, 0.32% pulmonary nodules, 0.92% emphysema, and 0.28% pulmonary embolism. The positive predictive values (PPVs) were: pneumothorax (0%), rib fractures (5.6%), aortic dilatation (43.2%), pulmonary emphysema (46.0%), pulmonary embolus (11.5%), and pulmonary nodules (9.2%). The PPV for pneumothorax was nil owing to lack of available studies that were analysed for outpatient activity.</p><p><strong>Conclusions: </strong>The number of missed findings was far less than generally predicted. The chest algorithms deployed retrospectively were a useful quality tool and AI augmented the radiologists' workflow.</p><p><strong>Advances in knowledge: </strong>The diagnostic accuracy of our radiologists generated missed findings of 0.02% for rib fractures CXR, 0.51% for aortic dilatation, 0.32% for pulmonary nodule, 0.92% for pulmonary emphysema, and 0.28% for pulmonary embolism for CT studies, all retrospectively evaluated with AI used as a quality tool to flag potential missed findings. It is important to account for prevalence of these chest conditions in clinical context and use appropriate clinical thresholds for decision-making, not relying solely on AI.</p>\",\"PeriodicalId\":72419,\"journal\":{\"name\":\"BJR open\",\"volume\":\"6 1\",\"pages\":\"tzad009\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2023-12-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10860529/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BJR open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/bjro/tzad009\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BJR open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/bjro/tzad009","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
A real-world evaluation of the diagnostic accuracy of radiologists using positive predictive values verified from deep learning and natural language processing chest algorithms deployed retrospectively.
Objectives: This diagnostic study assessed the accuracy of radiologists retrospectively, using the deep learning and natural language processing chest algorithms implemented in Clinical Review version 3.2 for: pneumothorax, rib fractures in digital chest X-ray radiographs (CXR); aortic aneurysm, pulmonary nodules, emphysema, and pulmonary embolism in CT images.
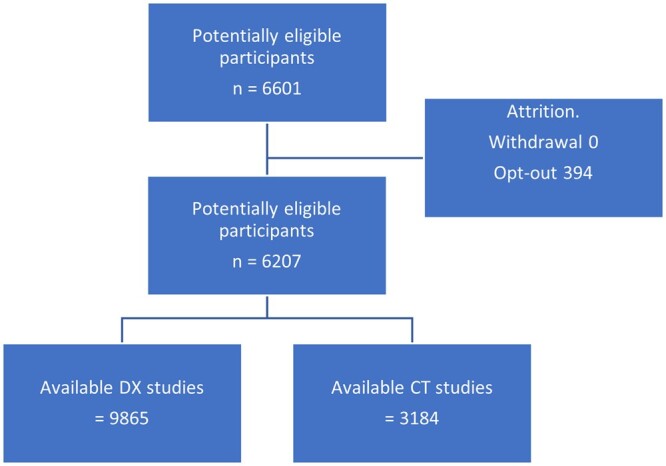
Methods: The study design was double-blind (artificial intelligence [AI] algorithms and humans), retrospective, non-interventional, and at a single NHS Trust. Adult patients (≥18 years old) scheduled for CXR and CT were invited to enroll as participants through an opt-out process. Reports and images were de-identified, processed retrospectively, and AI-flagged discrepant findings were assigned to two lead radiologists, each blinded to patient identifiers and original radiologist. The radiologist's findings for each clinical condition were tallied as a verified discrepancy (true positive) or not (false positive).
Results: The missed findings were: 0.02% rib fractures, 0.51% aortic aneurysm, 0.32% pulmonary nodules, 0.92% emphysema, and 0.28% pulmonary embolism. The positive predictive values (PPVs) were: pneumothorax (0%), rib fractures (5.6%), aortic dilatation (43.2%), pulmonary emphysema (46.0%), pulmonary embolus (11.5%), and pulmonary nodules (9.2%). The PPV for pneumothorax was nil owing to lack of available studies that were analysed for outpatient activity.
Conclusions: The number of missed findings was far less than generally predicted. The chest algorithms deployed retrospectively were a useful quality tool and AI augmented the radiologists' workflow.
Advances in knowledge: The diagnostic accuracy of our radiologists generated missed findings of 0.02% for rib fractures CXR, 0.51% for aortic dilatation, 0.32% for pulmonary nodule, 0.92% for pulmonary emphysema, and 0.28% for pulmonary embolism for CT studies, all retrospectively evaluated with AI used as a quality tool to flag potential missed findings. It is important to account for prevalence of these chest conditions in clinical context and use appropriate clinical thresholds for decision-making, not relying solely on AI.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


