Cristian Surcel, Robert Dotzauer, Cristian Mirvald, Calin Popa, Cosmin Olariu, Catalin Baston, Mihai Harza, Constantin Gangu, Igor Tsaur, Ioanel Sinescu
{"title":"术中细胞挽救技术在治疗伴有 III 和 IV 级下腔静脉血栓扩展的肾肿瘤中的当前作用。","authors":"Cristian Surcel, Robert Dotzauer, Cristian Mirvald, Calin Popa, Cosmin Olariu, Catalin Baston, Mihai Harza, Constantin Gangu, Igor Tsaur, Ioanel Sinescu","doi":"10.1177/17562872241229248","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>En bloc removal of the kidney with tumor thrombus excision in a multidisciplinary team remains the standard treatment for renal cell carcinoma (RCC) with tumor thrombus extension. In order to minimize the hemodynamic impact of the surgical blood loss, intraoperative cell salvage (IOCS) techniques can decrease the need for allogeneic blood and prevent blood transfusion related complications.</p><p><strong>Objective: </strong>In this article, we evaluated the safety of IOCS during radical nephrectomy with inferior vena cava thrombectomy under cardiopulmonary bypass with or without deep hypothermic circulatory arrest.</p><p><strong>Design and method: </strong>In this retrospective comparative multicenter analysis, clinical characteristics of 27 consecutive patients who underwent surgery with or without IOCS between 2012 and 2022 in three referral care units were collected into a database. The need for an allogenic blood transfusion (ABT) was also recorded, defined as any transfusion that occurred either intraoperatively or during the hospital stay.</p><p><strong>Results: </strong>The need for ABT in the cell saver arm was significantly smaller due to the reinfusion of rescued blood (<i>p</i> < 0.015). In multivariate analysis, no cell saver usage was an independent predictor for complications ⩾3 Clavien 3a [odds ratio (OR) 18.71, 95% CI 1.056-331.703, <i>p</i> = 0.046]. No usage of IOCS was an independent predictor for a lower risk of death (OR 0.277, 95% CI 0.062-0.825, <i>p</i> = 0.024). During follow-up, patients who received salvaged blood did not experience an increased risk for developing local recurrence or distant metastases.</p><p><strong>Conclusion: </strong>Transfusion of autologous blood is safe and can be using during nephrectomy and thrombectomy for advanced RCC.</p>","PeriodicalId":23010,"journal":{"name":"Therapeutic Advances in Urology","volume":"16 ","pages":"17562872241229248"},"PeriodicalIF":3.5000,"publicationDate":"2024-02-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10851714/pdf/","citationCount":"0","resultStr":"{\"title\":\"Current role of intraoperative cell salvage techniques in the management of renal tumors with level III and IV inferior vena cava thrombus extension.\",\"authors\":\"Cristian Surcel, Robert Dotzauer, Cristian Mirvald, Calin Popa, Cosmin Olariu, Catalin Baston, Mihai Harza, Constantin Gangu, Igor Tsaur, Ioanel Sinescu\",\"doi\":\"10.1177/17562872241229248\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>En bloc removal of the kidney with tumor thrombus excision in a multidisciplinary team remains the standard treatment for renal cell carcinoma (RCC) with tumor thrombus extension. In order to minimize the hemodynamic impact of the surgical blood loss, intraoperative cell salvage (IOCS) techniques can decrease the need for allogeneic blood and prevent blood transfusion related complications.</p><p><strong>Objective: </strong>In this article, we evaluated the safety of IOCS during radical nephrectomy with inferior vena cava thrombectomy under cardiopulmonary bypass with or without deep hypothermic circulatory arrest.</p><p><strong>Design and method: </strong>In this retrospective comparative multicenter analysis, clinical characteristics of 27 consecutive patients who underwent surgery with or without IOCS between 2012 and 2022 in three referral care units were collected into a database. The need for an allogenic blood transfusion (ABT) was also recorded, defined as any transfusion that occurred either intraoperatively or during the hospital stay.</p><p><strong>Results: </strong>The need for ABT in the cell saver arm was significantly smaller due to the reinfusion of rescued blood (<i>p</i> < 0.015). In multivariate analysis, no cell saver usage was an independent predictor for complications ⩾3 Clavien 3a [odds ratio (OR) 18.71, 95% CI 1.056-331.703, <i>p</i> = 0.046]. No usage of IOCS was an independent predictor for a lower risk of death (OR 0.277, 95% CI 0.062-0.825, <i>p</i> = 0.024). During follow-up, patients who received salvaged blood did not experience an increased risk for developing local recurrence or distant metastases.</p><p><strong>Conclusion: </strong>Transfusion of autologous blood is safe and can be using during nephrectomy and thrombectomy for advanced RCC.</p>\",\"PeriodicalId\":23010,\"journal\":{\"name\":\"Therapeutic Advances in Urology\",\"volume\":\"16 \",\"pages\":\"17562872241229248\"},\"PeriodicalIF\":3.5000,\"publicationDate\":\"2024-02-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10851714/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Therapeutic Advances in Urology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/17562872241229248\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Urology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/17562872241229248","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
Current role of intraoperative cell salvage techniques in the management of renal tumors with level III and IV inferior vena cava thrombus extension.
Background: En bloc removal of the kidney with tumor thrombus excision in a multidisciplinary team remains the standard treatment for renal cell carcinoma (RCC) with tumor thrombus extension. In order to minimize the hemodynamic impact of the surgical blood loss, intraoperative cell salvage (IOCS) techniques can decrease the need for allogeneic blood and prevent blood transfusion related complications.
Objective: In this article, we evaluated the safety of IOCS during radical nephrectomy with inferior vena cava thrombectomy under cardiopulmonary bypass with or without deep hypothermic circulatory arrest.
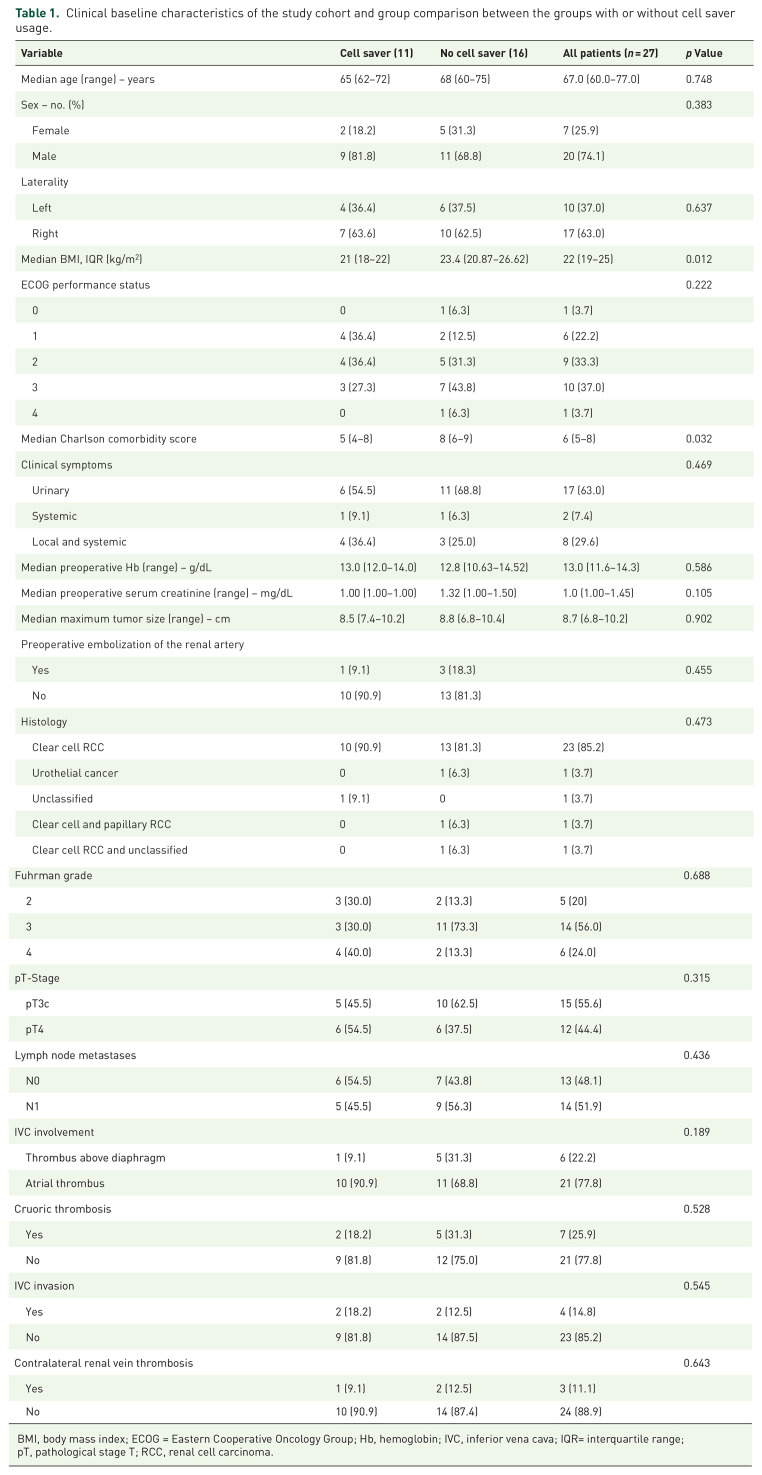
Design and method: In this retrospective comparative multicenter analysis, clinical characteristics of 27 consecutive patients who underwent surgery with or without IOCS between 2012 and 2022 in three referral care units were collected into a database. The need for an allogenic blood transfusion (ABT) was also recorded, defined as any transfusion that occurred either intraoperatively or during the hospital stay.
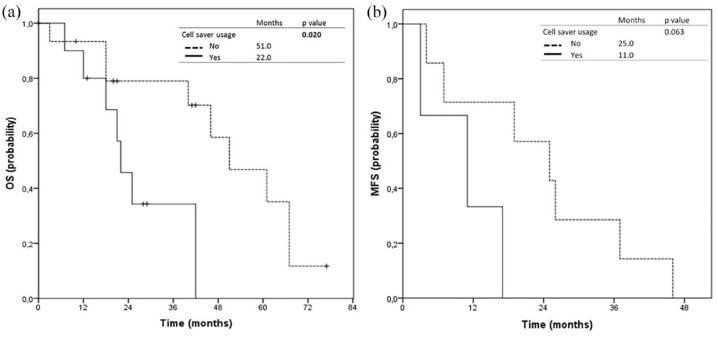
Results: The need for ABT in the cell saver arm was significantly smaller due to the reinfusion of rescued blood (p < 0.015). In multivariate analysis, no cell saver usage was an independent predictor for complications ⩾3 Clavien 3a [odds ratio (OR) 18.71, 95% CI 1.056-331.703, p = 0.046]. No usage of IOCS was an independent predictor for a lower risk of death (OR 0.277, 95% CI 0.062-0.825, p = 0.024). During follow-up, patients who received salvaged blood did not experience an increased risk for developing local recurrence or distant metastases.
Conclusion: Transfusion of autologous blood is safe and can be using during nephrectomy and thrombectomy for advanced RCC.
期刊介绍:
Therapeutic Advances in Urology delivers the highest quality peer-reviewed articles, reviews, and scholarly comment on pioneering efforts and innovative studies across all areas of urology.
The journal has a strong clinical and pharmacological focus and is aimed at clinicians and researchers in urology, providing a forum in print and online for publishing the highest quality articles in this area. The editors welcome articles of current interest across all areas of urology, including treatment of urological disorders, with a focus on emerging pharmacological therapies.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


