{"title":"无菌性、无创伤、药物难治性脑静脉窦血栓形成的机械取栓术:系统性综述。","authors":"John B Quealy","doi":"10.1007/s00062-023-01373-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cerebral venous sinus thrombosis (CVST) follows a severe clinical course in 13.5% of cases. Practice guidelines recommend endovascular therapy (EVT); no randomised control trials (RCTs) exist comparing EVTs.</p><p><strong>Purpose: </strong>To determine whether specific EVTs are superior to alternatives.</p><p><strong>Data sources: </strong>CENTRAL, Medline, Embase, five other databases and four clinical trials registers. Grey literature searches, reference checking, citation searching, and author contact.</p><p><strong>Study selection: </strong>All CVST cases treated with mechanical thrombectomy (MT) were includible. Paediatric, and trauma-related or infection-related thromboses were excluded.</p><p><strong>Data analysis: </strong>Standard Cochrane review procedures. Primary outcome measures; clinical efficacy (modified Rankin Score, mRS), technical efficacy (recanalisation), and clinical safety (procedure-related complications and death). Subgroup analyses were performed, comparing outcome measures between demographic groups, clinico-radiological severity, interventional strategies, and degrees of recanalisation.</p><p><strong>Data synthesis: </strong>In this study 124 papers were included (n = 486). All patients underwent MT, with 69.5% of patients receiving concomitant chemolysis. New/expanding intracerebral haemorrhage (ICH) occurred in 5.1%; non-haemorrhagic complications in 1.4%; 10.7% died. Predictors of poor efficacy included age ≥ 55 years, altered mental status (AMS), Glasgow Coma Scale (GCS) < 8. Predictive of poor safety outcomes included pre-existing ICH, deep system thrombosis, and AMS. Complete recanalisation was associated with improved clinical efficacy and safety outcomes.</p><p><strong>Limitations: </strong>The review is based on case reports/series, increasing bias-risk. Myriad of potentially includible studies were necessarily excluded due to lack of requisite details.</p><p><strong>Conclusion: </strong>Predictors of poor outcomes with medical therapy predict poor outcomes with MT; these measures should not dictate candidacy. Complete recanalisation predicts favorable clinical and safety outcomes. Local chemolysis is safe, improves recanalisation, and should be recommended, provided there is no contraindication. Clot maceration strategies and stent-retriever thrombectomy are associated with superior clinical efficacy and safety endpoints, as compared with balloon angioplasty and rheolysis.</p>","PeriodicalId":49298,"journal":{"name":"Clinical Neuroradiology","volume":" ","pages":"451-463"},"PeriodicalIF":2.6000,"publicationDate":"2024-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Mechanical Thrombectomy for Aseptic, Atraumatic, Medically Refractory Cerebral Venous Sinus Thrombosis: a Systematic Review.\",\"authors\":\"John B Quealy\",\"doi\":\"10.1007/s00062-023-01373-0\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Cerebral venous sinus thrombosis (CVST) follows a severe clinical course in 13.5% of cases. Practice guidelines recommend endovascular therapy (EVT); no randomised control trials (RCTs) exist comparing EVTs.</p><p><strong>Purpose: </strong>To determine whether specific EVTs are superior to alternatives.</p><p><strong>Data sources: </strong>CENTRAL, Medline, Embase, five other databases and four clinical trials registers. Grey literature searches, reference checking, citation searching, and author contact.</p><p><strong>Study selection: </strong>All CVST cases treated with mechanical thrombectomy (MT) were includible. Paediatric, and trauma-related or infection-related thromboses were excluded.</p><p><strong>Data analysis: </strong>Standard Cochrane review procedures. Primary outcome measures; clinical efficacy (modified Rankin Score, mRS), technical efficacy (recanalisation), and clinical safety (procedure-related complications and death). Subgroup analyses were performed, comparing outcome measures between demographic groups, clinico-radiological severity, interventional strategies, and degrees of recanalisation.</p><p><strong>Data synthesis: </strong>In this study 124 papers were included (n = 486). All patients underwent MT, with 69.5% of patients receiving concomitant chemolysis. New/expanding intracerebral haemorrhage (ICH) occurred in 5.1%; non-haemorrhagic complications in 1.4%; 10.7% died. Predictors of poor efficacy included age ≥ 55 years, altered mental status (AMS), Glasgow Coma Scale (GCS) < 8. Predictive of poor safety outcomes included pre-existing ICH, deep system thrombosis, and AMS. Complete recanalisation was associated with improved clinical efficacy and safety outcomes.</p><p><strong>Limitations: </strong>The review is based on case reports/series, increasing bias-risk. Myriad of potentially includible studies were necessarily excluded due to lack of requisite details.</p><p><strong>Conclusion: </strong>Predictors of poor outcomes with medical therapy predict poor outcomes with MT; these measures should not dictate candidacy. Complete recanalisation predicts favorable clinical and safety outcomes. Local chemolysis is safe, improves recanalisation, and should be recommended, provided there is no contraindication. Clot maceration strategies and stent-retriever thrombectomy are associated with superior clinical efficacy and safety endpoints, as compared with balloon angioplasty and rheolysis.</p>\",\"PeriodicalId\":49298,\"journal\":{\"name\":\"Clinical Neuroradiology\",\"volume\":\" \",\"pages\":\"451-463\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2024-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Neuroradiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s00062-023-01373-0\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/2/8 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Neuroradiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00062-023-01373-0","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/2/8 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Mechanical Thrombectomy for Aseptic, Atraumatic, Medically Refractory Cerebral Venous Sinus Thrombosis: a Systematic Review.
Background: Cerebral venous sinus thrombosis (CVST) follows a severe clinical course in 13.5% of cases. Practice guidelines recommend endovascular therapy (EVT); no randomised control trials (RCTs) exist comparing EVTs.
Purpose: To determine whether specific EVTs are superior to alternatives.
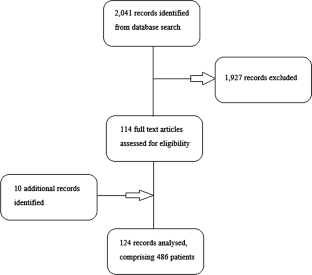
Data sources: CENTRAL, Medline, Embase, five other databases and four clinical trials registers. Grey literature searches, reference checking, citation searching, and author contact.
Study selection: All CVST cases treated with mechanical thrombectomy (MT) were includible. Paediatric, and trauma-related or infection-related thromboses were excluded.
Data analysis: Standard Cochrane review procedures. Primary outcome measures; clinical efficacy (modified Rankin Score, mRS), technical efficacy (recanalisation), and clinical safety (procedure-related complications and death). Subgroup analyses were performed, comparing outcome measures between demographic groups, clinico-radiological severity, interventional strategies, and degrees of recanalisation.
Data synthesis: In this study 124 papers were included (n = 486). All patients underwent MT, with 69.5% of patients receiving concomitant chemolysis. New/expanding intracerebral haemorrhage (ICH) occurred in 5.1%; non-haemorrhagic complications in 1.4%; 10.7% died. Predictors of poor efficacy included age ≥ 55 years, altered mental status (AMS), Glasgow Coma Scale (GCS) < 8. Predictive of poor safety outcomes included pre-existing ICH, deep system thrombosis, and AMS. Complete recanalisation was associated with improved clinical efficacy and safety outcomes.
Limitations: The review is based on case reports/series, increasing bias-risk. Myriad of potentially includible studies were necessarily excluded due to lack of requisite details.
Conclusion: Predictors of poor outcomes with medical therapy predict poor outcomes with MT; these measures should not dictate candidacy. Complete recanalisation predicts favorable clinical and safety outcomes. Local chemolysis is safe, improves recanalisation, and should be recommended, provided there is no contraindication. Clot maceration strategies and stent-retriever thrombectomy are associated with superior clinical efficacy and safety endpoints, as compared with balloon angioplasty and rheolysis.
期刊介绍:
Clinical Neuroradiology provides current information, original contributions, and reviews in the field of neuroradiology. An interdisciplinary approach is accomplished by diagnostic and therapeutic contributions related to associated subjects.
The international coverage and relevance of the journal is underlined by its being the official journal of the German, Swiss, and Austrian Societies of Neuroradiology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


