{"title":"左心房低电压区与肺静脉隔绝术治疗心房颤动时诱发和复发巨跳动房性心动过速之间的关系","authors":"Koichiro Sonoda, Tadatomo Fukushima, Asumi Takei, Kaishi Otsuka, Shiro Hata, Hiroki Shinboku, Takahiro Muroya, Koji Maemura","doi":"10.1007/s10840-024-01760-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The relationship between induction and recurrence due to atrial tachycardia (AT) and left atrial (LA) matrix progression after atrial fibrillation (AF) ablation remains unclear.</p><p><strong>Methods: </strong>One hundred fifty-two consecutive patients with paroxysmal and persistent AF who underwent pulmonary vein isolation (PVI) and cavo-tricuspid isthmus (CTI) ablation and achieved sinus rhythm before the procedure were classified into three groups according to the AT pattern induced after the procedure: group N (non-induced), F (focal pattern), and M (macroreentrant pattern) in 3D mapping.</p><p><strong>Results: </strong>The total rate of AT induction was 19.7% (30/152) in groups F (n = 13) and M (n = 17). Patients in group M were older than those in groups N and F, with higher CHADS<sub>2</sub>/CHA<sub>2</sub>DS<sub>2</sub>-VASc values, left atrial enlargement, and low-voltage area (LVA) size of LA. The receiver operating characteristic curve determined that the cut-off LVA for macroreentrant AT induction was 8.8 cm<sup>2</sup> (area under the curve [AUC]: 0.86, 95% confidence interval [CI]: 0.75-0.97). The recurrence of AT at 36 months in group N was 4.1% (5/122), and at the second ablation, all patients had macroreentrant AT. Patients with AT recurrence in group N had a wide LVA at the first ablation, and the cut-off LVA for AT recurrence was 6.5 cm<sup>2</sup> (AUC 0.94, 95%CI 0.88-0.99). Adjusted multivariate analysis showed that only LVA size was associated with the recurrence of macroreentrant AT (odds ratio 1.21, 95%CI 1.04-1.51).</p><p><strong>Conclusions: </strong>It is important to develop a therapeutic strategy based on the LVA size to suppress the recurrence of AT in these patients.</p>","PeriodicalId":16202,"journal":{"name":"Journal of Interventional Cardiac Electrophysiology","volume":null,"pages":null},"PeriodicalIF":2.1000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11288992/pdf/","citationCount":"0","resultStr":"{\"title\":\"Association between left atrial low-voltage area and induction and recurrence of macroreentrant atrial tachycardia in pulmonary vein isolation for atrial fibrillation.\",\"authors\":\"Koichiro Sonoda, Tadatomo Fukushima, Asumi Takei, Kaishi Otsuka, Shiro Hata, Hiroki Shinboku, Takahiro Muroya, Koji Maemura\",\"doi\":\"10.1007/s10840-024-01760-8\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The relationship between induction and recurrence due to atrial tachycardia (AT) and left atrial (LA) matrix progression after atrial fibrillation (AF) ablation remains unclear.</p><p><strong>Methods: </strong>One hundred fifty-two consecutive patients with paroxysmal and persistent AF who underwent pulmonary vein isolation (PVI) and cavo-tricuspid isthmus (CTI) ablation and achieved sinus rhythm before the procedure were classified into three groups according to the AT pattern induced after the procedure: group N (non-induced), F (focal pattern), and M (macroreentrant pattern) in 3D mapping.</p><p><strong>Results: </strong>The total rate of AT induction was 19.7% (30/152) in groups F (n = 13) and M (n = 17). Patients in group M were older than those in groups N and F, with higher CHADS<sub>2</sub>/CHA<sub>2</sub>DS<sub>2</sub>-VASc values, left atrial enlargement, and low-voltage area (LVA) size of LA. The receiver operating characteristic curve determined that the cut-off LVA for macroreentrant AT induction was 8.8 cm<sup>2</sup> (area under the curve [AUC]: 0.86, 95% confidence interval [CI]: 0.75-0.97). The recurrence of AT at 36 months in group N was 4.1% (5/122), and at the second ablation, all patients had macroreentrant AT. Patients with AT recurrence in group N had a wide LVA at the first ablation, and the cut-off LVA for AT recurrence was 6.5 cm<sup>2</sup> (AUC 0.94, 95%CI 0.88-0.99). Adjusted multivariate analysis showed that only LVA size was associated with the recurrence of macroreentrant AT (odds ratio 1.21, 95%CI 1.04-1.51).</p><p><strong>Conclusions: </strong>It is important to develop a therapeutic strategy based on the LVA size to suppress the recurrence of AT in these patients.</p>\",\"PeriodicalId\":16202,\"journal\":{\"name\":\"Journal of Interventional Cardiac Electrophysiology\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2024-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11288992/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Interventional Cardiac Electrophysiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s10840-024-01760-8\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/2/6 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Interventional Cardiac Electrophysiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10840-024-01760-8","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/2/6 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
背景:房颤(AF)消融术后房性心动过速(AT)和左心房(LA)基质进展导致的诱发和复发之间的关系仍不清楚:方法:对连续接受肺静脉隔离(PVI)和腔静脉-三尖瓣峡部(CTI)消融术且术前达到窦性心律的152例阵发性和持续性房颤患者,根据术后诱发的房颤模式将其分为三组:N组(非诱发)、F组(局灶模式)和M组(三维映射下的大返流模式):F 组(13 人)和 M 组(17 人)的 AT 诱导总比率为 19.7%(30/152)。M组患者年龄大于N组和F组,CHADS2/CHA2DS2-VASc值、左心房增大和LA低电压区(LVA)大小均高于N组和F组。根据接收者操作特征曲线确定,大回旋诱导 AT 的 LVA 临界值为 8.8 平方厘米(曲线下面积 [AUC]:0.86,95% 置信区间 [CI]:0.75-0.97)。N 组患者在 36 个月时 AT 复发率为 4.1%(5/122),在第二次消融时,所有患者的 AT 均为大回缩。N组AT复发患者在第一次消融时LVA较宽,AT复发的临界LVA为6.5平方厘米(AUC 0.94,95%CI 0.88-0.99)。调整后的多变量分析显示,只有LVA的大小与大再障AT的复发有关(几率比1.21,95%CI 1.04-1.51):结论:根据LVA大小制定治疗策略以抑制这些患者的AT复发非常重要。
Association between left atrial low-voltage area and induction and recurrence of macroreentrant atrial tachycardia in pulmonary vein isolation for atrial fibrillation.
Background: The relationship between induction and recurrence due to atrial tachycardia (AT) and left atrial (LA) matrix progression after atrial fibrillation (AF) ablation remains unclear.
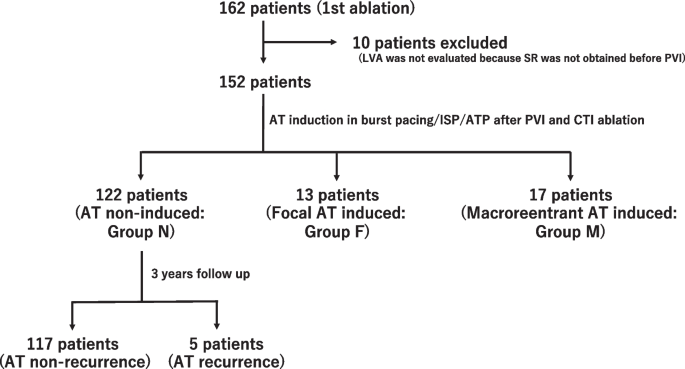
Methods: One hundred fifty-two consecutive patients with paroxysmal and persistent AF who underwent pulmonary vein isolation (PVI) and cavo-tricuspid isthmus (CTI) ablation and achieved sinus rhythm before the procedure were classified into three groups according to the AT pattern induced after the procedure: group N (non-induced), F (focal pattern), and M (macroreentrant pattern) in 3D mapping.
Results: The total rate of AT induction was 19.7% (30/152) in groups F (n = 13) and M (n = 17). Patients in group M were older than those in groups N and F, with higher CHADS2/CHA2DS2-VASc values, left atrial enlargement, and low-voltage area (LVA) size of LA. The receiver operating characteristic curve determined that the cut-off LVA for macroreentrant AT induction was 8.8 cm2 (area under the curve [AUC]: 0.86, 95% confidence interval [CI]: 0.75-0.97). The recurrence of AT at 36 months in group N was 4.1% (5/122), and at the second ablation, all patients had macroreentrant AT. Patients with AT recurrence in group N had a wide LVA at the first ablation, and the cut-off LVA for AT recurrence was 6.5 cm2 (AUC 0.94, 95%CI 0.88-0.99). Adjusted multivariate analysis showed that only LVA size was associated with the recurrence of macroreentrant AT (odds ratio 1.21, 95%CI 1.04-1.51).
Conclusions: It is important to develop a therapeutic strategy based on the LVA size to suppress the recurrence of AT in these patients.
期刊介绍:
The Journal of Interventional Cardiac Electrophysiology is an international publication devoted to fostering research in and development of interventional techniques and therapies for the management of cardiac arrhythmias. It is designed primarily to present original research studies and scholarly scientific reviews of basic and applied science and clinical research in this field. The Journal will adopt a multidisciplinary approach to link physical, experimental, and clinical sciences as applied to the development of and practice in interventional electrophysiology. The Journal will examine techniques ranging from molecular, chemical and pharmacologic therapies to device and ablation technology. Accordingly, original research in clinical, epidemiologic and basic science arenas will be considered for publication. Applied engineering or physical science studies pertaining to interventional electrophysiology will be encouraged. The Journal is committed to providing comprehensive and detailed treatment of major interventional therapies and innovative techniques in a structured and clinically relevant manner. It is directed at clinical practitioners and investigators in the rapidly growing field of interventional electrophysiology. The editorial staff and board reflect this bias and include noted international experts in this area with a wealth of expertise in basic and clinical investigation. Peer review of all submissions, conflict of interest guidelines and periodic editorial board review of all Journal policies have been established.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


