Kenta Nakase, Ryosuke Matsuda, Shoh Sasaki, Ichiro Nakagawa
{"title":"林奇综合征相关胶质母细胞瘤同时接受化放疗和免疫检查点抑制剂治疗:病例报告和文献综述。","authors":"Kenta Nakase, Ryosuke Matsuda, Shoh Sasaki, Ichiro Nakagawa","doi":"10.14791/btrt.2023.0042","DOIUrl":null,"url":null,"abstract":"<p><p>Lynch syndrome (LS) is an autosomal dominant disorder caused by mutations in mismatch repair (MMR) genes and is also known to be associated with glioblastomas. The efficacy of immunotherapy for LS-associated glioblastomas remains unknown. Herein, we report a rare case of LS-associated glioblastoma, treated with chemotherapy using immune checkpoint inhibitors (ICI). A 41-year-old female patient presented with headaches and sensory disturbances in the right upper limb for 6 weeks. She had been treated for rectal cancer and had a family history of LS. MRI revealed two ring-enhancing lesions in the left precentral gyrus. She underwent subtotal resection, leading to a pathological diagnosis of isocitrate dehydrogenase wild-type glioblastoma. She received daily administration of (temozolomide, 75 mg/m²) and concurrent radiotherapy (60 Gy) postoperatively. However, the tumor recurred 1 year after the initial treatment. A molecular genetic study showed high microsatellite instability (MSI), and she was treated with pembrolizumab therapy. Disease progression occurred despite six cycles of pembrolizumab therapy and radiotherapy at the dose of 40 Gy. She died due to glioblastoma progression 19 months after the initial treatment. The present case demonstrates that some LS-associated glioblastomas may be resistant to ICI despite high MSI, possibly because of intratumor heterogeneity related to MMR deficiency.</p>","PeriodicalId":72453,"journal":{"name":"Brain tumor research and treatment","volume":"12 1","pages":"70-74"},"PeriodicalIF":0.0000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10864134/pdf/","citationCount":"0","resultStr":"{\"title\":\"Lynch Syndrome-Associated Glioblastoma Treated With Concomitant Chemoradiotherapy and Immune Checkpoint Inhibitors: Case Report and Review of Literature.\",\"authors\":\"Kenta Nakase, Ryosuke Matsuda, Shoh Sasaki, Ichiro Nakagawa\",\"doi\":\"10.14791/btrt.2023.0042\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Lynch syndrome (LS) is an autosomal dominant disorder caused by mutations in mismatch repair (MMR) genes and is also known to be associated with glioblastomas. The efficacy of immunotherapy for LS-associated glioblastomas remains unknown. Herein, we report a rare case of LS-associated glioblastoma, treated with chemotherapy using immune checkpoint inhibitors (ICI). A 41-year-old female patient presented with headaches and sensory disturbances in the right upper limb for 6 weeks. She had been treated for rectal cancer and had a family history of LS. MRI revealed two ring-enhancing lesions in the left precentral gyrus. She underwent subtotal resection, leading to a pathological diagnosis of isocitrate dehydrogenase wild-type glioblastoma. She received daily administration of (temozolomide, 75 mg/m²) and concurrent radiotherapy (60 Gy) postoperatively. However, the tumor recurred 1 year after the initial treatment. A molecular genetic study showed high microsatellite instability (MSI), and she was treated with pembrolizumab therapy. Disease progression occurred despite six cycles of pembrolizumab therapy and radiotherapy at the dose of 40 Gy. She died due to glioblastoma progression 19 months after the initial treatment. The present case demonstrates that some LS-associated glioblastomas may be resistant to ICI despite high MSI, possibly because of intratumor heterogeneity related to MMR deficiency.</p>\",\"PeriodicalId\":72453,\"journal\":{\"name\":\"Brain tumor research and treatment\",\"volume\":\"12 1\",\"pages\":\"70-74\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10864134/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Brain tumor research and treatment\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14791/btrt.2023.0042\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Brain tumor research and treatment","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14791/btrt.2023.0042","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Lynch Syndrome-Associated Glioblastoma Treated With Concomitant Chemoradiotherapy and Immune Checkpoint Inhibitors: Case Report and Review of Literature.
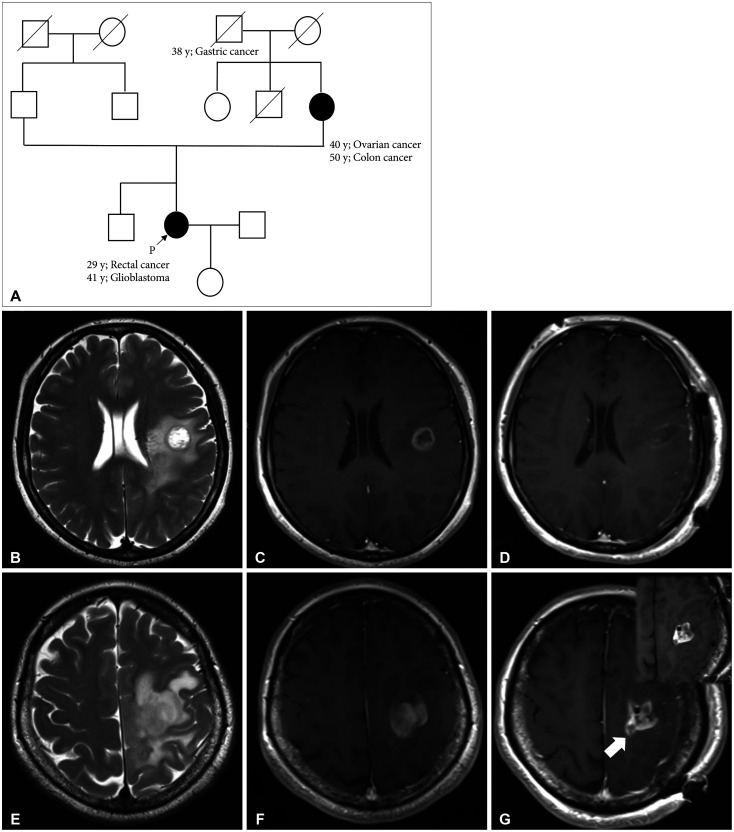
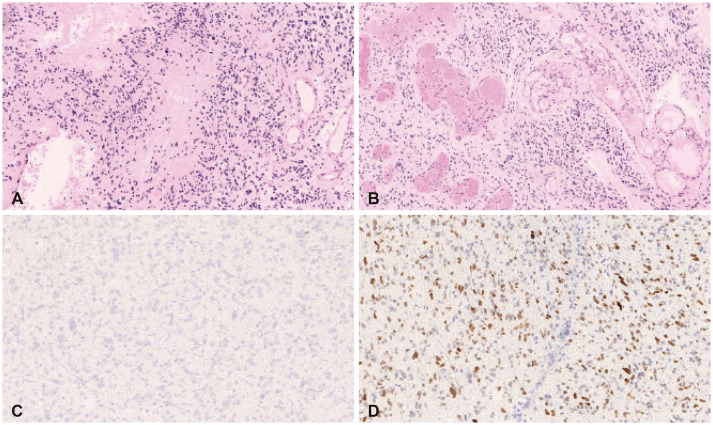
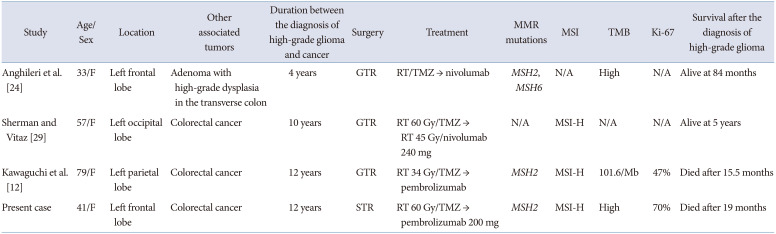
Lynch syndrome (LS) is an autosomal dominant disorder caused by mutations in mismatch repair (MMR) genes and is also known to be associated with glioblastomas. The efficacy of immunotherapy for LS-associated glioblastomas remains unknown. Herein, we report a rare case of LS-associated glioblastoma, treated with chemotherapy using immune checkpoint inhibitors (ICI). A 41-year-old female patient presented with headaches and sensory disturbances in the right upper limb for 6 weeks. She had been treated for rectal cancer and had a family history of LS. MRI revealed two ring-enhancing lesions in the left precentral gyrus. She underwent subtotal resection, leading to a pathological diagnosis of isocitrate dehydrogenase wild-type glioblastoma. She received daily administration of (temozolomide, 75 mg/m²) and concurrent radiotherapy (60 Gy) postoperatively. However, the tumor recurred 1 year after the initial treatment. A molecular genetic study showed high microsatellite instability (MSI), and she was treated with pembrolizumab therapy. Disease progression occurred despite six cycles of pembrolizumab therapy and radiotherapy at the dose of 40 Gy. She died due to glioblastoma progression 19 months after the initial treatment. The present case demonstrates that some LS-associated glioblastomas may be resistant to ICI despite high MSI, possibly because of intratumor heterogeneity related to MMR deficiency.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


