{"title":"代谢健康肥胖的短暂性:代谢衰退与动脉粥样硬化风险","authors":"Saeid Mirzai, Ian J. Neeland, Carl J. Lavie","doi":"10.1002/dmrr.3765","DOIUrl":null,"url":null,"abstract":"<p>The concept of metabolically healthy obesity (MHO)—obesity in the absence of metabolic abnormalities such as hypertension, dyslipidemia, and hyperglycemia—has sparked intense debate.<span><sup>1</sup></span> Up to 40% of people with obesity exhibit an MHO phenotype, seemingly escaping obesity's expected cardiometabolic sequelae.<span><sup>2</sup></span> But is this a real phenomenon with a persistent favourable prognosis, or does MHO reflect a transient phenotype bound to become metabolically unhealthy with associated cardiovascular disease (CVD) consequences?</p><p>In this issue of the journal, Huang et al. provide data to support the latter premise.<span><sup>3</sup></span> The authors present an analysis of 50,885 middle-aged and elderly Chinese adults that examined the association between weight/metabolic phenotypes and subclinical atherosclerosis. Based on cutoffs from Chinese guidelines, participants were stratified by body mass index (BMI) into normal weight, overweight, or obesity. Metabolic health status was defined as healthy (0–2 of 5 metabolic abnormalities) or unhealthy (≥3 of 5 abnormalities) using the International Diabetes Federation criteria. Outcomes studied included early (increased carotid intima-media thickness [CIMT]), intermediate (plaques), and late (stenosis >50%) stage carotid atherosclerotic changes along with a composite of the three, termed carotid atherosclerosis.</p><p>Their key findings were that metabolically unhealthy groups, irrespective of BMI category, had significantly heightened odds for carotid atherosclerosis compared with their healthy counterparts with similar BMI. This affirms metabolic disorders as the primary drivers of vascular disease rather than obesity itself. Still, participants with MHO (4.7% of participants) showed 10% higher odds for carotid atherosclerosis than healthy normal weight individuals after adjustment (adjusted odds ratio 1.10, 95% confidence interval [CI] 1.02–1.21), driven primarily by higher odds of increased CIMT (Figure 1). These findings remained significant in men and younger (≤60 years) participants with MHO but not their counterparts. Most strikingly, 33.4% of baseline metabolically healthy participants who were living with overweight or obesity developed metabolic abnormalities within the 2-year follow-up. These ‘converters’ had a 21% higher risk of carotid atherosclerosis than those maintaining stable healthy status over time (adjusted hazard ratio 1.21, 95% CI 1.02–1.43) (Figure 1).</p><p>The authors are applauded for a sophisticated study benefiting from a large, well-characterised cohort across a spectrum of body weight and metabolic parameters. Repeated health surveys enabled the evaluation of transitions from health to disease, and the characterisation of multi-stage carotid changes helped time-course understanding. However, some limitations exist. The exclusively Chinese population may restrict generalisability, and cardiorespiratory fitness (CRF) measures were unavailable—a particular limitation given unusually high self-reported physical activity levels across all groups (∼60% reporting regular exercise), raising validity concerns regarding these questionnaire data. Yet, the take-home message is clear–metabolic health matters more than obesity for atherosclerosis, but excess weight still elevates risks even if other biomarkers remain normal. And most importantly, the MHO state appears transient for many.</p><p>These latest findings feed into the ongoing controversial debates about the existence and prognosis of MHO.<span><sup>4</sup></span> The differing definitions of metabolic health (no consensus with up to 30 distinct criteria used in the literature), variations in study follow-up periods, and range of endpoints evaluated across cohorts have contributed to conflicting results.<span><sup>5, 6</sup></span> While strong associations exist between excess weight and conditions like heart failure and atrial fibrillation, atherosclerosis and coronary artery disease appear more linked to metabolic abnormalities than body weight.<span><sup>7, 8</sup></span> This study supports that relationship, given the stronger relationship between metabolic abnormalities and carotid atherosclerosis, but the lack of sensitivity analyses using different metabolic health cutoffs is a limitation. Notably, beyond subclinical disease measures, a 2013 meta-analysis showed MHO has a modestly increased risk for CVD events (relative risk 1.24, 95% CI 1.02–1.55) compared to metabolically healthy normal weight individuals in studies with ≥10 years of follow-up.<span><sup>9</sup></span> This suggests that increased weight, even without metabolic abnormalities, carries long-term CVD risks.</p><p>Also, like this study, the current literature paints a consistent picture that MHO largely represents a transient state rather than a durable phenotype. While some individuals maintain metabolic health despite obesity over time, between one-third to one-half convert to metabolically unhealthy status when followed for up to 10 years<span><sup>6</sup></span> Over even longer periods, this conversion percentage grows—with only 16% and 6% of women with initial MHO retaining healthy metrics at 20 and 30 years, respectively, in the Nurses' Health Study.<span><sup>10</sup></span> Greater visceral fat, declining insulin sensitivity, worsening inflammation, and lifestyle factors appear to predict progression from MHO to unhealthy.<span><sup>6</sup></span> The analysis by Huang et al. showed that over 30% of MHO Chinese adults transitioned to metabolically unhealthy within just 2 years. Although longer tracking of this cohort would likely have revealed a greater rise in metabolic abnormality onsets and atherosclerotic risks, the findings should raise major concerns given their significance despite relatively short follow-up.</p><p>The question remains of what to do with these findings. Returning to the major limitation of a lack of standard definition for MHO, the residual CVD risk seen in the MHO subgroup may be concentrated on those predisposed by factors like lifestyle factors, body fat distribution, or inflammatory tendencies.<span><sup>6</sup></span> Hence, augmenting metabolic criteria with more precise markers of adipose dysfunction could better risk-stratify this group. More importantly, future research efforts could help identify predictors of metabolic health decline over time in this group for implementation of interventions targeting modifiable factors like diet, CRF, and stress to stabilise the MHO phenotype.<span><sup>6</sup></span> Identifying and mitigating modifiable determinants of metabolic health loss could guide efforts to prevent progression and maintain the better prognosis of MHO.</p><p>But potentially no factor may matter more than CRF for CVD outcomes across the weight strata.<span><sup>11</sup></span> Past research has indicated that taking CRF into consideration can modify the association between MHO and clinical or subclinical CVD.<span><sup>12-15</sup></span> This suggests that CRF assessments are sorely lacking yet much needed in research on MHO phenotypes. Demonstrating whether CRF gains can offset risks linked to otherwise healthy obesity could strongly influence clinical practice. If achievable through lifestyle counselling and exercise programs, improving CRF could provide superior benefits to pursuing weight loss for risk mitigation in this population. Assessing CRF and the impact of improving it on CVD outcomes should be a priority in future MHO studies.</p><p>In summary, the study by Huang et al. provides compelling evidence for MHO as an at-risk state for subclinical vascular disease. Although not as detrimental as unhealthy obesity, healthy overweight/obesity still carried elevated odds for carotid atherosclerosis, which increased with the sizeable conversion rate to abnormal metabolic status over 2 years. Thus, losing excess weight remains prudent clinical advice for population health gains, even among those currently spared metabolic abnormalities. However, further investigations of MHO using more detailed criteria could help identify subgroups with particular advantages that mitigate the risks associated with obesity.</p><p>All authors contributed equally to the manuscript, including conceptualisation, drafting, editing, and final approval.</p><p>Dr. Lavie serves on a DSMB for NovoNordisk for their REDEFINE 3 Trial with CagriSema. Drs. Mirzai and Neeland have no relationships with the industry relevant to this paper to disclose.</p><p>National Heart, Lung, and Blood Institute of the National Institutes of Health, Grant/Award Number:T32HL076132</p>","PeriodicalId":11335,"journal":{"name":"Diabetes/Metabolism Research and Reviews","volume":"40 2","pages":""},"PeriodicalIF":4.6000,"publicationDate":"2024-02-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/dmrr.3765","citationCount":"0","resultStr":"{\"title\":\"The transiency of metabolically healthy obesity: Metabolic decline and atherosclerotic risk\",\"authors\":\"Saeid Mirzai, Ian J. Neeland, Carl J. Lavie\",\"doi\":\"10.1002/dmrr.3765\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>The concept of metabolically healthy obesity (MHO)—obesity in the absence of metabolic abnormalities such as hypertension, dyslipidemia, and hyperglycemia—has sparked intense debate.<span><sup>1</sup></span> Up to 40% of people with obesity exhibit an MHO phenotype, seemingly escaping obesity's expected cardiometabolic sequelae.<span><sup>2</sup></span> But is this a real phenomenon with a persistent favourable prognosis, or does MHO reflect a transient phenotype bound to become metabolically unhealthy with associated cardiovascular disease (CVD) consequences?</p><p>In this issue of the journal, Huang et al. provide data to support the latter premise.<span><sup>3</sup></span> The authors present an analysis of 50,885 middle-aged and elderly Chinese adults that examined the association between weight/metabolic phenotypes and subclinical atherosclerosis. Based on cutoffs from Chinese guidelines, participants were stratified by body mass index (BMI) into normal weight, overweight, or obesity. Metabolic health status was defined as healthy (0–2 of 5 metabolic abnormalities) or unhealthy (≥3 of 5 abnormalities) using the International Diabetes Federation criteria. Outcomes studied included early (increased carotid intima-media thickness [CIMT]), intermediate (plaques), and late (stenosis >50%) stage carotid atherosclerotic changes along with a composite of the three, termed carotid atherosclerosis.</p><p>Their key findings were that metabolically unhealthy groups, irrespective of BMI category, had significantly heightened odds for carotid atherosclerosis compared with their healthy counterparts with similar BMI. This affirms metabolic disorders as the primary drivers of vascular disease rather than obesity itself. Still, participants with MHO (4.7% of participants) showed 10% higher odds for carotid atherosclerosis than healthy normal weight individuals after adjustment (adjusted odds ratio 1.10, 95% confidence interval [CI] 1.02–1.21), driven primarily by higher odds of increased CIMT (Figure 1). These findings remained significant in men and younger (≤60 years) participants with MHO but not their counterparts. Most strikingly, 33.4% of baseline metabolically healthy participants who were living with overweight or obesity developed metabolic abnormalities within the 2-year follow-up. These ‘converters’ had a 21% higher risk of carotid atherosclerosis than those maintaining stable healthy status over time (adjusted hazard ratio 1.21, 95% CI 1.02–1.43) (Figure 1).</p><p>The authors are applauded for a sophisticated study benefiting from a large, well-characterised cohort across a spectrum of body weight and metabolic parameters. Repeated health surveys enabled the evaluation of transitions from health to disease, and the characterisation of multi-stage carotid changes helped time-course understanding. However, some limitations exist. The exclusively Chinese population may restrict generalisability, and cardiorespiratory fitness (CRF) measures were unavailable—a particular limitation given unusually high self-reported physical activity levels across all groups (∼60% reporting regular exercise), raising validity concerns regarding these questionnaire data. Yet, the take-home message is clear–metabolic health matters more than obesity for atherosclerosis, but excess weight still elevates risks even if other biomarkers remain normal. And most importantly, the MHO state appears transient for many.</p><p>These latest findings feed into the ongoing controversial debates about the existence and prognosis of MHO.<span><sup>4</sup></span> The differing definitions of metabolic health (no consensus with up to 30 distinct criteria used in the literature), variations in study follow-up periods, and range of endpoints evaluated across cohorts have contributed to conflicting results.<span><sup>5, 6</sup></span> While strong associations exist between excess weight and conditions like heart failure and atrial fibrillation, atherosclerosis and coronary artery disease appear more linked to metabolic abnormalities than body weight.<span><sup>7, 8</sup></span> This study supports that relationship, given the stronger relationship between metabolic abnormalities and carotid atherosclerosis, but the lack of sensitivity analyses using different metabolic health cutoffs is a limitation. Notably, beyond subclinical disease measures, a 2013 meta-analysis showed MHO has a modestly increased risk for CVD events (relative risk 1.24, 95% CI 1.02–1.55) compared to metabolically healthy normal weight individuals in studies with ≥10 years of follow-up.<span><sup>9</sup></span> This suggests that increased weight, even without metabolic abnormalities, carries long-term CVD risks.</p><p>Also, like this study, the current literature paints a consistent picture that MHO largely represents a transient state rather than a durable phenotype. While some individuals maintain metabolic health despite obesity over time, between one-third to one-half convert to metabolically unhealthy status when followed for up to 10 years<span><sup>6</sup></span> Over even longer periods, this conversion percentage grows—with only 16% and 6% of women with initial MHO retaining healthy metrics at 20 and 30 years, respectively, in the Nurses' Health Study.<span><sup>10</sup></span> Greater visceral fat, declining insulin sensitivity, worsening inflammation, and lifestyle factors appear to predict progression from MHO to unhealthy.<span><sup>6</sup></span> The analysis by Huang et al. showed that over 30% of MHO Chinese adults transitioned to metabolically unhealthy within just 2 years. Although longer tracking of this cohort would likely have revealed a greater rise in metabolic abnormality onsets and atherosclerotic risks, the findings should raise major concerns given their significance despite relatively short follow-up.</p><p>The question remains of what to do with these findings. Returning to the major limitation of a lack of standard definition for MHO, the residual CVD risk seen in the MHO subgroup may be concentrated on those predisposed by factors like lifestyle factors, body fat distribution, or inflammatory tendencies.<span><sup>6</sup></span> Hence, augmenting metabolic criteria with more precise markers of adipose dysfunction could better risk-stratify this group. More importantly, future research efforts could help identify predictors of metabolic health decline over time in this group for implementation of interventions targeting modifiable factors like diet, CRF, and stress to stabilise the MHO phenotype.<span><sup>6</sup></span> Identifying and mitigating modifiable determinants of metabolic health loss could guide efforts to prevent progression and maintain the better prognosis of MHO.</p><p>But potentially no factor may matter more than CRF for CVD outcomes across the weight strata.<span><sup>11</sup></span> Past research has indicated that taking CRF into consideration can modify the association between MHO and clinical or subclinical CVD.<span><sup>12-15</sup></span> This suggests that CRF assessments are sorely lacking yet much needed in research on MHO phenotypes. Demonstrating whether CRF gains can offset risks linked to otherwise healthy obesity could strongly influence clinical practice. If achievable through lifestyle counselling and exercise programs, improving CRF could provide superior benefits to pursuing weight loss for risk mitigation in this population. Assessing CRF and the impact of improving it on CVD outcomes should be a priority in future MHO studies.</p><p>In summary, the study by Huang et al. provides compelling evidence for MHO as an at-risk state for subclinical vascular disease. Although not as detrimental as unhealthy obesity, healthy overweight/obesity still carried elevated odds for carotid atherosclerosis, which increased with the sizeable conversion rate to abnormal metabolic status over 2 years. Thus, losing excess weight remains prudent clinical advice for population health gains, even among those currently spared metabolic abnormalities. However, further investigations of MHO using more detailed criteria could help identify subgroups with particular advantages that mitigate the risks associated with obesity.</p><p>All authors contributed equally to the manuscript, including conceptualisation, drafting, editing, and final approval.</p><p>Dr. Lavie serves on a DSMB for NovoNordisk for their REDEFINE 3 Trial with CagriSema. Drs. Mirzai and Neeland have no relationships with the industry relevant to this paper to disclose.</p><p>National Heart, Lung, and Blood Institute of the National Institutes of Health, Grant/Award Number:T32HL076132</p>\",\"PeriodicalId\":11335,\"journal\":{\"name\":\"Diabetes/Metabolism Research and Reviews\",\"volume\":\"40 2\",\"pages\":\"\"},\"PeriodicalIF\":4.6000,\"publicationDate\":\"2024-02-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/dmrr.3765\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Diabetes/Metabolism Research and Reviews\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/dmrr.3765\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Diabetes/Metabolism Research and Reviews","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/dmrr.3765","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
The transiency of metabolically healthy obesity: Metabolic decline and atherosclerotic risk
The concept of metabolically healthy obesity (MHO)—obesity in the absence of metabolic abnormalities such as hypertension, dyslipidemia, and hyperglycemia—has sparked intense debate.1 Up to 40% of people with obesity exhibit an MHO phenotype, seemingly escaping obesity's expected cardiometabolic sequelae.2 But is this a real phenomenon with a persistent favourable prognosis, or does MHO reflect a transient phenotype bound to become metabolically unhealthy with associated cardiovascular disease (CVD) consequences?
In this issue of the journal, Huang et al. provide data to support the latter premise.3 The authors present an analysis of 50,885 middle-aged and elderly Chinese adults that examined the association between weight/metabolic phenotypes and subclinical atherosclerosis. Based on cutoffs from Chinese guidelines, participants were stratified by body mass index (BMI) into normal weight, overweight, or obesity. Metabolic health status was defined as healthy (0–2 of 5 metabolic abnormalities) or unhealthy (≥3 of 5 abnormalities) using the International Diabetes Federation criteria. Outcomes studied included early (increased carotid intima-media thickness [CIMT]), intermediate (plaques), and late (stenosis >50%) stage carotid atherosclerotic changes along with a composite of the three, termed carotid atherosclerosis.
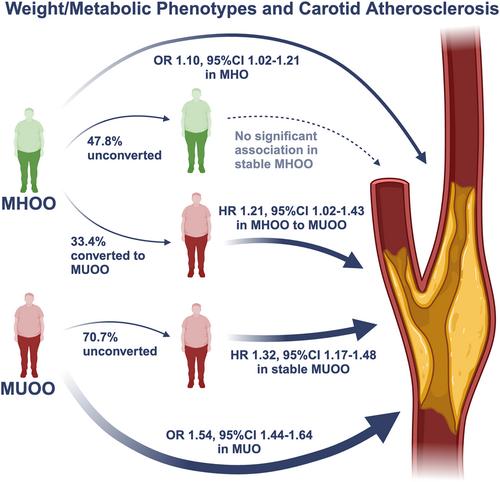
Their key findings were that metabolically unhealthy groups, irrespective of BMI category, had significantly heightened odds for carotid atherosclerosis compared with their healthy counterparts with similar BMI. This affirms metabolic disorders as the primary drivers of vascular disease rather than obesity itself. Still, participants with MHO (4.7% of participants) showed 10% higher odds for carotid atherosclerosis than healthy normal weight individuals after adjustment (adjusted odds ratio 1.10, 95% confidence interval [CI] 1.02–1.21), driven primarily by higher odds of increased CIMT (Figure 1). These findings remained significant in men and younger (≤60 years) participants with MHO but not their counterparts. Most strikingly, 33.4% of baseline metabolically healthy participants who were living with overweight or obesity developed metabolic abnormalities within the 2-year follow-up. These ‘converters’ had a 21% higher risk of carotid atherosclerosis than those maintaining stable healthy status over time (adjusted hazard ratio 1.21, 95% CI 1.02–1.43) (Figure 1).
The authors are applauded for a sophisticated study benefiting from a large, well-characterised cohort across a spectrum of body weight and metabolic parameters. Repeated health surveys enabled the evaluation of transitions from health to disease, and the characterisation of multi-stage carotid changes helped time-course understanding. However, some limitations exist. The exclusively Chinese population may restrict generalisability, and cardiorespiratory fitness (CRF) measures were unavailable—a particular limitation given unusually high self-reported physical activity levels across all groups (∼60% reporting regular exercise), raising validity concerns regarding these questionnaire data. Yet, the take-home message is clear–metabolic health matters more than obesity for atherosclerosis, but excess weight still elevates risks even if other biomarkers remain normal. And most importantly, the MHO state appears transient for many.
These latest findings feed into the ongoing controversial debates about the existence and prognosis of MHO.4 The differing definitions of metabolic health (no consensus with up to 30 distinct criteria used in the literature), variations in study follow-up periods, and range of endpoints evaluated across cohorts have contributed to conflicting results.5, 6 While strong associations exist between excess weight and conditions like heart failure and atrial fibrillation, atherosclerosis and coronary artery disease appear more linked to metabolic abnormalities than body weight.7, 8 This study supports that relationship, given the stronger relationship between metabolic abnormalities and carotid atherosclerosis, but the lack of sensitivity analyses using different metabolic health cutoffs is a limitation. Notably, beyond subclinical disease measures, a 2013 meta-analysis showed MHO has a modestly increased risk for CVD events (relative risk 1.24, 95% CI 1.02–1.55) compared to metabolically healthy normal weight individuals in studies with ≥10 years of follow-up.9 This suggests that increased weight, even without metabolic abnormalities, carries long-term CVD risks.
Also, like this study, the current literature paints a consistent picture that MHO largely represents a transient state rather than a durable phenotype. While some individuals maintain metabolic health despite obesity over time, between one-third to one-half convert to metabolically unhealthy status when followed for up to 10 years6 Over even longer periods, this conversion percentage grows—with only 16% and 6% of women with initial MHO retaining healthy metrics at 20 and 30 years, respectively, in the Nurses' Health Study.10 Greater visceral fat, declining insulin sensitivity, worsening inflammation, and lifestyle factors appear to predict progression from MHO to unhealthy.6 The analysis by Huang et al. showed that over 30% of MHO Chinese adults transitioned to metabolically unhealthy within just 2 years. Although longer tracking of this cohort would likely have revealed a greater rise in metabolic abnormality onsets and atherosclerotic risks, the findings should raise major concerns given their significance despite relatively short follow-up.
The question remains of what to do with these findings. Returning to the major limitation of a lack of standard definition for MHO, the residual CVD risk seen in the MHO subgroup may be concentrated on those predisposed by factors like lifestyle factors, body fat distribution, or inflammatory tendencies.6 Hence, augmenting metabolic criteria with more precise markers of adipose dysfunction could better risk-stratify this group. More importantly, future research efforts could help identify predictors of metabolic health decline over time in this group for implementation of interventions targeting modifiable factors like diet, CRF, and stress to stabilise the MHO phenotype.6 Identifying and mitigating modifiable determinants of metabolic health loss could guide efforts to prevent progression and maintain the better prognosis of MHO.
But potentially no factor may matter more than CRF for CVD outcomes across the weight strata.11 Past research has indicated that taking CRF into consideration can modify the association between MHO and clinical or subclinical CVD.12-15 This suggests that CRF assessments are sorely lacking yet much needed in research on MHO phenotypes. Demonstrating whether CRF gains can offset risks linked to otherwise healthy obesity could strongly influence clinical practice. If achievable through lifestyle counselling and exercise programs, improving CRF could provide superior benefits to pursuing weight loss for risk mitigation in this population. Assessing CRF and the impact of improving it on CVD outcomes should be a priority in future MHO studies.
In summary, the study by Huang et al. provides compelling evidence for MHO as an at-risk state for subclinical vascular disease. Although not as detrimental as unhealthy obesity, healthy overweight/obesity still carried elevated odds for carotid atherosclerosis, which increased with the sizeable conversion rate to abnormal metabolic status over 2 years. Thus, losing excess weight remains prudent clinical advice for population health gains, even among those currently spared metabolic abnormalities. However, further investigations of MHO using more detailed criteria could help identify subgroups with particular advantages that mitigate the risks associated with obesity.
All authors contributed equally to the manuscript, including conceptualisation, drafting, editing, and final approval.
Dr. Lavie serves on a DSMB for NovoNordisk for their REDEFINE 3 Trial with CagriSema. Drs. Mirzai and Neeland have no relationships with the industry relevant to this paper to disclose.
National Heart, Lung, and Blood Institute of the National Institutes of Health, Grant/Award Number:T32HL076132
期刊介绍:
Diabetes/Metabolism Research and Reviews is a premier endocrinology and metabolism journal esteemed by clinicians and researchers alike. Encompassing a wide spectrum of topics including diabetes, endocrinology, metabolism, and obesity, the journal eagerly accepts submissions ranging from clinical studies to basic and translational research, as well as reviews exploring historical progress, controversial issues, and prominent opinions in the field. Join us in advancing knowledge and understanding in the realm of diabetes and metabolism.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


