{"title":"右美托咪定促进无插管视频辅助胸腔镜手术后的恢复","authors":"","doi":"10.1016/j.jfma.2024.01.017","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>Non-intubated video-assisted thoracoscopic surgery combines a minimally invasive technique with multimodal locoregional analgesia to enhance recovery. The mainstay sedation protocol involves propofol and fentanyl. Dexmedetomidine, given its opioid-sparing effect with minimal respiratory depression, facilitates sedation in non-intubated patients. This study aimed to evaluate the efficacy of dexmedetomidine during non-intubated video-assisted thoracoscopic surgery.</p></div><div><h3>Methods</h3><p>A total of 114 patients who underwent non-intubated video-assisted thoracoscopic surgery between June 2015 and September 2017 were retrospectively evaluated. Of these, 34 were maintained with dexmedetomidine, propofol, and fentanyl, and 80 were maintained with propofol and fentanyl. After a 1:1 propensity score-matched analysis incorporating sex, body mass index, American Society of Anesthesiologists classification, pulmonary disease and hypertension, the clinical outcomes of 34 pairs of patients were assessed.</p></div><div><h3>Results</h3><p>The dexmedetomidine group showed a significantly lower opioid consumption [10.3 (5.7–15.1) vs. 18.8 (10.0–31.0) mg, median (interquartile range); <em>P</em> = 0.001] on postoperative day 0 and a significantly shorter postoperative length of stay [3 (2–4) vs. 4 (3–5) days, median (interquartile range), <em>P</em> = 0.006] than the control group. During operation, the proportion of vasopressor administration was significantly higher in the dexmedetomidine group [18 (53) vs. 7 (21), patient number (%), <em>P</em> = 0.01]. On the other hand, the difference of the hypotension and bradycardia incidence, short-term morbidity and mortality rates between each group were nonsignificant.</p></div><div><h3>Conclusion</h3><p>Adding adjuvant dexmedetomidine to propofol and fentanyl is safe and feasible for non-intubated video-assisted thoracoscopic surgery. With its opioid-sparing effect and shorter postoperative length of stay, dexmedetomidine may enhance recovery after surgery.</p></div>","PeriodicalId":17305,"journal":{"name":"Journal of the Formosan Medical Association","volume":"123 9","pages":"Pages 961-967"},"PeriodicalIF":2.6000,"publicationDate":"2024-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.sciencedirect.com/science/article/pii/S0929664624000500/pdfft?md5=3cbe59267686e0abd79b3a4c99310af5&pid=1-s2.0-S0929664624000500-main.pdf","citationCount":"0","resultStr":"{\"title\":\"Dexmedetomidine for enhanced recovery after non-intubated video-assisted thoracoscopic surgery\",\"authors\":\"\",\"doi\":\"10.1016/j.jfma.2024.01.017\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background</h3><p>Non-intubated video-assisted thoracoscopic surgery combines a minimally invasive technique with multimodal locoregional analgesia to enhance recovery. The mainstay sedation protocol involves propofol and fentanyl. Dexmedetomidine, given its opioid-sparing effect with minimal respiratory depression, facilitates sedation in non-intubated patients. This study aimed to evaluate the efficacy of dexmedetomidine during non-intubated video-assisted thoracoscopic surgery.</p></div><div><h3>Methods</h3><p>A total of 114 patients who underwent non-intubated video-assisted thoracoscopic surgery between June 2015 and September 2017 were retrospectively evaluated. Of these, 34 were maintained with dexmedetomidine, propofol, and fentanyl, and 80 were maintained with propofol and fentanyl. After a 1:1 propensity score-matched analysis incorporating sex, body mass index, American Society of Anesthesiologists classification, pulmonary disease and hypertension, the clinical outcomes of 34 pairs of patients were assessed.</p></div><div><h3>Results</h3><p>The dexmedetomidine group showed a significantly lower opioid consumption [10.3 (5.7–15.1) vs. 18.8 (10.0–31.0) mg, median (interquartile range); <em>P</em> = 0.001] on postoperative day 0 and a significantly shorter postoperative length of stay [3 (2–4) vs. 4 (3–5) days, median (interquartile range), <em>P</em> = 0.006] than the control group. During operation, the proportion of vasopressor administration was significantly higher in the dexmedetomidine group [18 (53) vs. 7 (21), patient number (%), <em>P</em> = 0.01]. On the other hand, the difference of the hypotension and bradycardia incidence, short-term morbidity and mortality rates between each group were nonsignificant.</p></div><div><h3>Conclusion</h3><p>Adding adjuvant dexmedetomidine to propofol and fentanyl is safe and feasible for non-intubated video-assisted thoracoscopic surgery. With its opioid-sparing effect and shorter postoperative length of stay, dexmedetomidine may enhance recovery after surgery.</p></div>\",\"PeriodicalId\":17305,\"journal\":{\"name\":\"Journal of the Formosan Medical Association\",\"volume\":\"123 9\",\"pages\":\"Pages 961-967\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2024-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.sciencedirect.com/science/article/pii/S0929664624000500/pdfft?md5=3cbe59267686e0abd79b3a4c99310af5&pid=1-s2.0-S0929664624000500-main.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the Formosan Medical Association\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S0929664624000500\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the Formosan Medical Association","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0929664624000500","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
摘要
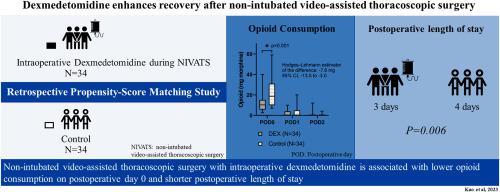
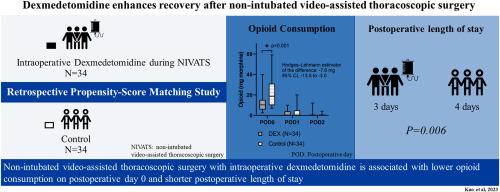
背景无插管视频辅助胸腔镜手术结合了微创技术和多模式局部镇痛,以促进术后恢复。主流镇静方案包括异丙酚和芬太尼。右美托咪定具有节省阿片类药物的作用,且呼吸抑制极小,有助于非插管患者的镇静。本研究旨在评估右美托咪定在非插管视频辅助胸腔镜手术中的疗效。方法回顾性评估了2015年6月至2017年9月期间接受非插管视频辅助胸腔镜手术的114例患者。其中,34 名患者使用右美托咪定、异丙酚和芬太尼维持治疗,80 名患者使用异丙酚和芬太尼维持治疗。根据性别、体重指数、美国麻醉学会分类、肺部疾病和高血压进行 1:1 倾向评分匹配分析后,对 34 对患者的临床结果进行了评估。术后第 0 天,右美托咪定组的阿片类药物消耗量明显低于对照组[10.3(5.7-15.1)毫克 vs. 18.8(10.0-31.0)毫克,中位数(四分位数间距);P = 0.001],术后住院时间明显短于对照组[3(2-4)天 vs. 4(3-5)天,中位数(四分位数间距),P = 0.006]。在手术过程中,右美托咪定组使用血管加压药的比例明显高于对照组 [18 (53) vs. 7 (21),患者人数(%),P = 0.01]。结论在异丙酚和芬太尼的基础上添加右美托咪定辅助治疗,对于非插管的视频辅助胸腔镜手术是安全可行的。右美托咪定具有节省阿片类药物和缩短术后住院时间的作用,可促进术后恢复。
Dexmedetomidine for enhanced recovery after non-intubated video-assisted thoracoscopic surgery
Background
Non-intubated video-assisted thoracoscopic surgery combines a minimally invasive technique with multimodal locoregional analgesia to enhance recovery. The mainstay sedation protocol involves propofol and fentanyl. Dexmedetomidine, given its opioid-sparing effect with minimal respiratory depression, facilitates sedation in non-intubated patients. This study aimed to evaluate the efficacy of dexmedetomidine during non-intubated video-assisted thoracoscopic surgery.
Methods
A total of 114 patients who underwent non-intubated video-assisted thoracoscopic surgery between June 2015 and September 2017 were retrospectively evaluated. Of these, 34 were maintained with dexmedetomidine, propofol, and fentanyl, and 80 were maintained with propofol and fentanyl. After a 1:1 propensity score-matched analysis incorporating sex, body mass index, American Society of Anesthesiologists classification, pulmonary disease and hypertension, the clinical outcomes of 34 pairs of patients were assessed.
Results
The dexmedetomidine group showed a significantly lower opioid consumption [10.3 (5.7–15.1) vs. 18.8 (10.0–31.0) mg, median (interquartile range); P = 0.001] on postoperative day 0 and a significantly shorter postoperative length of stay [3 (2–4) vs. 4 (3–5) days, median (interquartile range), P = 0.006] than the control group. During operation, the proportion of vasopressor administration was significantly higher in the dexmedetomidine group [18 (53) vs. 7 (21), patient number (%), P = 0.01]. On the other hand, the difference of the hypotension and bradycardia incidence, short-term morbidity and mortality rates between each group were nonsignificant.
Conclusion
Adding adjuvant dexmedetomidine to propofol and fentanyl is safe and feasible for non-intubated video-assisted thoracoscopic surgery. With its opioid-sparing effect and shorter postoperative length of stay, dexmedetomidine may enhance recovery after surgery.
期刊介绍:
Journal of the Formosan Medical Association (JFMA), published continuously since 1902, is an open access international general medical journal of the Formosan Medical Association based in Taipei, Taiwan. It is indexed in Current Contents/ Clinical Medicine, Medline, ciSearch, CAB Abstracts, Embase, SIIC Data Bases, Research Alert, BIOSIS, Biological Abstracts, Scopus and ScienceDirect.
As a general medical journal, research related to clinical practice and research in all fields of medicine and related disciplines are considered for publication. Article types considered include perspectives, reviews, original papers, case reports, brief communications, correspondence and letters to the editor.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


