Julie K.K. Vishram-Nielsen MD, PhD , Fernando Luis Scolari MD, PhD , Chun-Po Steve Fan PhD , Yas Moayedi MD , Heather J. Ross MD, MHSc , Cedric Manlhiot PhD , Melissa A. Allwood MD, PhD , Ana Carolina Alba MD, PhD , Keith R. Brunt PhD , Jeremy A. Simpson PhD , Filio Billia MD, PhD
{"title":"利用中枢作用疗法改善心力衰竭患者的呼吸功能。","authors":"Julie K.K. Vishram-Nielsen MD, PhD , Fernando Luis Scolari MD, PhD , Chun-Po Steve Fan PhD , Yas Moayedi MD , Heather J. Ross MD, MHSc , Cedric Manlhiot PhD , Melissa A. Allwood MD, PhD , Ana Carolina Alba MD, PhD , Keith R. Brunt PhD , Jeremy A. Simpson PhD , Filio Billia MD, PhD","doi":"10.1016/j.cjco.2024.01.003","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>Diaphragm atrophy can contribute to dyspnea in patients with heart failure (HF) with its link to central neurohormonal overactivation. HF medications that cross the blood-brain barrier could act centrally and improve respiratory function, potentially alleviating diaphragmatic atrophy. Therefore, we compared the benefit of central- vs peripheral-acting HF drugs on respiratory function, as assessed by a single cardiopulmonary exercise test (CPET) and outcomes in HF patients.</p></div><div><h3>Methods</h3><p>A retrospective study was conducted of 624 ambulatory adult HF patients (80% male) with reduced left ventricular ejection fraction ≤ 40% and a complete CPET, followed at a single institution between 2001 and 2017. CPET parameters, and the outcomes all-cause death, a composite endpoint (all-cause death, need for left ventricular assist device, heart transplantation), and all-cause and/or HF hospitalizations, were compared in patients receiving central-acting (n = 550) vs peripheral-acting (n = 74) drugs.</p></div><div><h3>Results</h3><p>Compared to patients who receive peripheral-acting drugs, patients who receive central-acting drugs had better respiratory function (peak breath-by breath oxygen uptake [VO<sub>2</sub>], <em>P</em> = 0.020; forced expiratory volume in 1 second [FEV1], <em>P</em> = 0.007), and ventilatory efficiency (minute ventilation / carbon dioxide production [VE/VCO<sub>2</sub>], <em>P</em> < 0.001; end-tidal carbon dioxide tension [PETCO<sub>2</sub>], <em>P</em> = 0.015; and trend for forced vital capacity [FVC], <em>P</em> = 0.056). Many of the associations between the CPET parameters and drug type remained significant after multivariate adjustment. Moreover, patients receiving central-acting drugs had fewer composite events (<em>P</em> = 0.023), and HF hospitalizations (<em>P</em> = 0.044), although significance after multivariant correction was not achieved, despite the hazard ratio being 0.664 and 0.757, respectively.</p></div><div><h3>Conclusions</h3><p>Central-acting drugs were associated with better respiratory function as measured by CPET parameters in HF patients. This could extend to clinically meaningful composite outcomes and hospitalizations but required more power to be definitive in linking to drug effect. Central-acting HF drugs show a role in mitigating diaphragm weakness.</p></div>","PeriodicalId":36924,"journal":{"name":"CJC Open","volume":"6 5","pages":"Pages 745-754"},"PeriodicalIF":2.5000,"publicationDate":"2024-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.sciencedirect.com/science/article/pii/S2589790X24000246/pdfft?md5=17508265fa99001010df60e7f6fdc99f&pid=1-s2.0-S2589790X24000246-main.pdf","citationCount":"0","resultStr":"{\"title\":\"Better Respiratory Function in Heart Failure Patients With Use of Central-Acting Therapeutics\",\"authors\":\"Julie K.K. Vishram-Nielsen MD, PhD , Fernando Luis Scolari MD, PhD , Chun-Po Steve Fan PhD , Yas Moayedi MD , Heather J. Ross MD, MHSc , Cedric Manlhiot PhD , Melissa A. Allwood MD, PhD , Ana Carolina Alba MD, PhD , Keith R. Brunt PhD , Jeremy A. Simpson PhD , Filio Billia MD, PhD\",\"doi\":\"10.1016/j.cjco.2024.01.003\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background</h3><p>Diaphragm atrophy can contribute to dyspnea in patients with heart failure (HF) with its link to central neurohormonal overactivation. HF medications that cross the blood-brain barrier could act centrally and improve respiratory function, potentially alleviating diaphragmatic atrophy. Therefore, we compared the benefit of central- vs peripheral-acting HF drugs on respiratory function, as assessed by a single cardiopulmonary exercise test (CPET) and outcomes in HF patients.</p></div><div><h3>Methods</h3><p>A retrospective study was conducted of 624 ambulatory adult HF patients (80% male) with reduced left ventricular ejection fraction ≤ 40% and a complete CPET, followed at a single institution between 2001 and 2017. CPET parameters, and the outcomes all-cause death, a composite endpoint (all-cause death, need for left ventricular assist device, heart transplantation), and all-cause and/or HF hospitalizations, were compared in patients receiving central-acting (n = 550) vs peripheral-acting (n = 74) drugs.</p></div><div><h3>Results</h3><p>Compared to patients who receive peripheral-acting drugs, patients who receive central-acting drugs had better respiratory function (peak breath-by breath oxygen uptake [VO<sub>2</sub>], <em>P</em> = 0.020; forced expiratory volume in 1 second [FEV1], <em>P</em> = 0.007), and ventilatory efficiency (minute ventilation / carbon dioxide production [VE/VCO<sub>2</sub>], <em>P</em> < 0.001; end-tidal carbon dioxide tension [PETCO<sub>2</sub>], <em>P</em> = 0.015; and trend for forced vital capacity [FVC], <em>P</em> = 0.056). Many of the associations between the CPET parameters and drug type remained significant after multivariate adjustment. Moreover, patients receiving central-acting drugs had fewer composite events (<em>P</em> = 0.023), and HF hospitalizations (<em>P</em> = 0.044), although significance after multivariant correction was not achieved, despite the hazard ratio being 0.664 and 0.757, respectively.</p></div><div><h3>Conclusions</h3><p>Central-acting drugs were associated with better respiratory function as measured by CPET parameters in HF patients. This could extend to clinically meaningful composite outcomes and hospitalizations but required more power to be definitive in linking to drug effect. Central-acting HF drugs show a role in mitigating diaphragm weakness.</p></div>\",\"PeriodicalId\":36924,\"journal\":{\"name\":\"CJC Open\",\"volume\":\"6 5\",\"pages\":\"Pages 745-754\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2024-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.sciencedirect.com/science/article/pii/S2589790X24000246/pdfft?md5=17508265fa99001010df60e7f6fdc99f&pid=1-s2.0-S2589790X24000246-main.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"CJC Open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2589790X24000246\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"CJC Open","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2589790X24000246","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Better Respiratory Function in Heart Failure Patients With Use of Central-Acting Therapeutics
Background
Diaphragm atrophy can contribute to dyspnea in patients with heart failure (HF) with its link to central neurohormonal overactivation. HF medications that cross the blood-brain barrier could act centrally and improve respiratory function, potentially alleviating diaphragmatic atrophy. Therefore, we compared the benefit of central- vs peripheral-acting HF drugs on respiratory function, as assessed by a single cardiopulmonary exercise test (CPET) and outcomes in HF patients.
Methods
A retrospective study was conducted of 624 ambulatory adult HF patients (80% male) with reduced left ventricular ejection fraction ≤ 40% and a complete CPET, followed at a single institution between 2001 and 2017. CPET parameters, and the outcomes all-cause death, a composite endpoint (all-cause death, need for left ventricular assist device, heart transplantation), and all-cause and/or HF hospitalizations, were compared in patients receiving central-acting (n = 550) vs peripheral-acting (n = 74) drugs.
Results
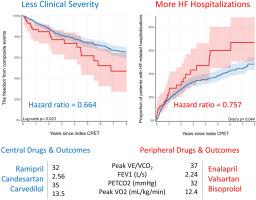
Compared to patients who receive peripheral-acting drugs, patients who receive central-acting drugs had better respiratory function (peak breath-by breath oxygen uptake [VO2], P = 0.020; forced expiratory volume in 1 second [FEV1], P = 0.007), and ventilatory efficiency (minute ventilation / carbon dioxide production [VE/VCO2], P < 0.001; end-tidal carbon dioxide tension [PETCO2], P = 0.015; and trend for forced vital capacity [FVC], P = 0.056). Many of the associations between the CPET parameters and drug type remained significant after multivariate adjustment. Moreover, patients receiving central-acting drugs had fewer composite events (P = 0.023), and HF hospitalizations (P = 0.044), although significance after multivariant correction was not achieved, despite the hazard ratio being 0.664 and 0.757, respectively.
Conclusions
Central-acting drugs were associated with better respiratory function as measured by CPET parameters in HF patients. This could extend to clinically meaningful composite outcomes and hospitalizations but required more power to be definitive in linking to drug effect. Central-acting HF drugs show a role in mitigating diaphragm weakness.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


