{"title":"急性髓性白血病,细胞学检查有误导。","authors":"Mayssa Gaaloul, Madalina Uzunov, Karim Maloum, Elise Sourdeau","doi":"10.1111/ijlh.14233","DOIUrl":null,"url":null,"abstract":"<p>A 78-year-old woman presented with asthenia and superficial bleeding. Blood tests revealed pancytopenia with neutropenia (0.38 × 10<sup>9</sup>/L), anemia (94 g/L), and thrombocytopenia (50 × 10<sup>9</sup>/L). The peripheral blood smear showed 9% immature hypergranular atypical cells morphologically looking like abnormal promyelocytes and frequently containing bundles of Auer rods (Figure 1A–C). No schistocytes were present. Hemostasis tests revealed features of disseminated intravascular coagulation with hypofibrinogenemia (0.6 g/L), elevated D-dimer (7038 mg/L), decreased factor V (61%), and prolonged prothrombin time (19.1 s). The activated partial thromboplastin time was normal (35.5 s). Bone marrow aspirate smear showed 24% cells morphologically looking like abnormal promyelocytes with bundles of Auer rods (Figure 1D), and moderate dysplasia (hypo or agranularity and some dystrophic megakaryocytes). Flow cytometry analysis identified a blastic population extending to the maturing granulocyte region, expressing CD45 (dim), CD33, CD13, cytoplasmic-myeloperoxidase and CD117 (dim) without CD34, HLA-DR or CD15 expression (Figure 2).</p><p>This clinical and biological presentation was consistent with acute promyelocytic leukemia (APL). She received a plasma transfusion and all-trans-retinoic acid. However, karyotyping and fluorescent <i>in situ</i> hybridization did not detect t(15;17) or any other abnormality. Molecular testing showed mutations of <i>TET2</i> (c.3729dup, 45%; c.3409+2T>A, 49%), <i>SRSF2</i> (c.284C>A, 45%), and <i>BRAF</i> (c.1803A>T, 2%), but not <i>PML::RARA</i> rearrangement. These results excluded the diagnosis of APL and acute myeloid leukemia (AML) with dysplasia was retained. Treatment was switched and she received an induction chemotherapy with a combination of Idarubicine and cytarabine (“3 + 7”).</p><p>In this case, the cytopenias and the morphological abnormalities suggested AML with dysplasia, but morphology mimicked APL complicated with disseminated intravascular coagulation. Promyelocytes with bundles of Auer rods are characteristically found in APL but are not specific, being rarely reported in non-APL myeloid neoplasms. Only a few cases of AML mimicking APL have been reported. They often present with cytogenetic abnormalities [(inv)16, t(8;21), t(7;11), etc.].<span><sup>1, 2</sup></span> Our patient displayed normal karyotype but a myelodysplastic syndrome mutational profile. This case highlights the importance of rapid cytogenetic and molecular testing for an accurate characterisation of AML as recommended by World Health Organization,<span><sup>3</sup></span> to quickly initiate the appropriate treatment.</p><p>MG and ES collected all the biological data, MU and KM provided clinical data. All authors contributed to writing the manuscript.</p>","PeriodicalId":14120,"journal":{"name":"International Journal of Laboratory Hematology","volume":"46 4","pages":"583-584"},"PeriodicalIF":2.2000,"publicationDate":"2024-01-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/ijlh.14233","citationCount":"0","resultStr":"{\"title\":\"Acute myeloid leukemia with misleading cytology\",\"authors\":\"Mayssa Gaaloul, Madalina Uzunov, Karim Maloum, Elise Sourdeau\",\"doi\":\"10.1111/ijlh.14233\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>A 78-year-old woman presented with asthenia and superficial bleeding. Blood tests revealed pancytopenia with neutropenia (0.38 × 10<sup>9</sup>/L), anemia (94 g/L), and thrombocytopenia (50 × 10<sup>9</sup>/L). The peripheral blood smear showed 9% immature hypergranular atypical cells morphologically looking like abnormal promyelocytes and frequently containing bundles of Auer rods (Figure 1A–C). No schistocytes were present. Hemostasis tests revealed features of disseminated intravascular coagulation with hypofibrinogenemia (0.6 g/L), elevated D-dimer (7038 mg/L), decreased factor V (61%), and prolonged prothrombin time (19.1 s). The activated partial thromboplastin time was normal (35.5 s). Bone marrow aspirate smear showed 24% cells morphologically looking like abnormal promyelocytes with bundles of Auer rods (Figure 1D), and moderate dysplasia (hypo or agranularity and some dystrophic megakaryocytes). Flow cytometry analysis identified a blastic population extending to the maturing granulocyte region, expressing CD45 (dim), CD33, CD13, cytoplasmic-myeloperoxidase and CD117 (dim) without CD34, HLA-DR or CD15 expression (Figure 2).</p><p>This clinical and biological presentation was consistent with acute promyelocytic leukemia (APL). She received a plasma transfusion and all-trans-retinoic acid. However, karyotyping and fluorescent <i>in situ</i> hybridization did not detect t(15;17) or any other abnormality. Molecular testing showed mutations of <i>TET2</i> (c.3729dup, 45%; c.3409+2T>A, 49%), <i>SRSF2</i> (c.284C>A, 45%), and <i>BRAF</i> (c.1803A>T, 2%), but not <i>PML::RARA</i> rearrangement. These results excluded the diagnosis of APL and acute myeloid leukemia (AML) with dysplasia was retained. Treatment was switched and she received an induction chemotherapy with a combination of Idarubicine and cytarabine (“3 + 7”).</p><p>In this case, the cytopenias and the morphological abnormalities suggested AML with dysplasia, but morphology mimicked APL complicated with disseminated intravascular coagulation. Promyelocytes with bundles of Auer rods are characteristically found in APL but are not specific, being rarely reported in non-APL myeloid neoplasms. Only a few cases of AML mimicking APL have been reported. They often present with cytogenetic abnormalities [(inv)16, t(8;21), t(7;11), etc.].<span><sup>1, 2</sup></span> Our patient displayed normal karyotype but a myelodysplastic syndrome mutational profile. This case highlights the importance of rapid cytogenetic and molecular testing for an accurate characterisation of AML as recommended by World Health Organization,<span><sup>3</sup></span> to quickly initiate the appropriate treatment.</p><p>MG and ES collected all the biological data, MU and KM provided clinical data. All authors contributed to writing the manuscript.</p>\",\"PeriodicalId\":14120,\"journal\":{\"name\":\"International Journal of Laboratory Hematology\",\"volume\":\"46 4\",\"pages\":\"583-584\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2024-01-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/ijlh.14233\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Laboratory Hematology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/ijlh.14233\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Laboratory Hematology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/ijlh.14233","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"HEMATOLOGY","Score":null,"Total":0}
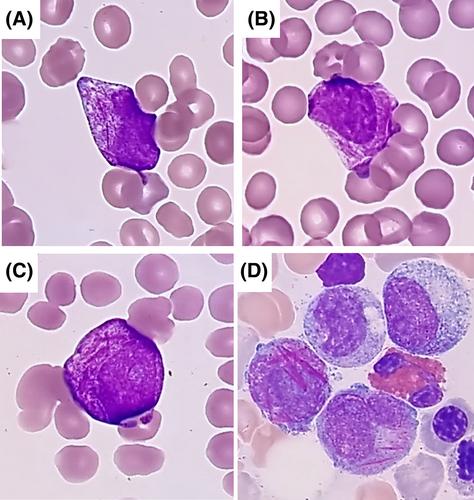
A 78-year-old woman presented with asthenia and superficial bleeding. Blood tests revealed pancytopenia with neutropenia (0.38 × 109/L), anemia (94 g/L), and thrombocytopenia (50 × 109/L). The peripheral blood smear showed 9% immature hypergranular atypical cells morphologically looking like abnormal promyelocytes and frequently containing bundles of Auer rods (Figure 1A–C). No schistocytes were present. Hemostasis tests revealed features of disseminated intravascular coagulation with hypofibrinogenemia (0.6 g/L), elevated D-dimer (7038 mg/L), decreased factor V (61%), and prolonged prothrombin time (19.1 s). The activated partial thromboplastin time was normal (35.5 s). Bone marrow aspirate smear showed 24% cells morphologically looking like abnormal promyelocytes with bundles of Auer rods (Figure 1D), and moderate dysplasia (hypo or agranularity and some dystrophic megakaryocytes). Flow cytometry analysis identified a blastic population extending to the maturing granulocyte region, expressing CD45 (dim), CD33, CD13, cytoplasmic-myeloperoxidase and CD117 (dim) without CD34, HLA-DR or CD15 expression (Figure 2).
This clinical and biological presentation was consistent with acute promyelocytic leukemia (APL). She received a plasma transfusion and all-trans-retinoic acid. However, karyotyping and fluorescent in situ hybridization did not detect t(15;17) or any other abnormality. Molecular testing showed mutations of TET2 (c.3729dup, 45%; c.3409+2T>A, 49%), SRSF2 (c.284C>A, 45%), and BRAF (c.1803A>T, 2%), but not PML::RARA rearrangement. These results excluded the diagnosis of APL and acute myeloid leukemia (AML) with dysplasia was retained. Treatment was switched and she received an induction chemotherapy with a combination of Idarubicine and cytarabine (“3 + 7”).
In this case, the cytopenias and the morphological abnormalities suggested AML with dysplasia, but morphology mimicked APL complicated with disseminated intravascular coagulation. Promyelocytes with bundles of Auer rods are characteristically found in APL but are not specific, being rarely reported in non-APL myeloid neoplasms. Only a few cases of AML mimicking APL have been reported. They often present with cytogenetic abnormalities [(inv)16, t(8;21), t(7;11), etc.].1, 2 Our patient displayed normal karyotype but a myelodysplastic syndrome mutational profile. This case highlights the importance of rapid cytogenetic and molecular testing for an accurate characterisation of AML as recommended by World Health Organization,3 to quickly initiate the appropriate treatment.
MG and ES collected all the biological data, MU and KM provided clinical data. All authors contributed to writing the manuscript.
期刊介绍:
The International Journal of Laboratory Hematology provides a forum for the communication of new developments, research topics and the practice of laboratory haematology.
The journal publishes invited reviews, full length original articles, and correspondence.
The International Journal of Laboratory Hematology is the official journal of the International Society for Laboratory Hematology, which addresses the following sub-disciplines: cellular analysis, flow cytometry, haemostasis and thrombosis, molecular diagnostics, haematology informatics, haemoglobinopathies, point of care testing, standards and guidelines.
The journal was launched in 2006 as the successor to Clinical and Laboratory Hematology, which was first published in 1979. An active and positive editorial policy ensures that work of a high scientific standard is reported, in order to bridge the gap between practical and academic aspects of laboratory haematology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


