Peter Calvert, Wern Yew Ding, Michael Griffin, Arnaud Bisson, Ioanna Koniari, Noel Fitzpatrick, Richard Snowdon, Simon Modi, Vishal Luther, Saagar Mahida, Johan Waktare, Zoltan Borbas, Reza Ashrafi, Derick Todd, Dhiraj Gupta
{"title":"心房颤动重做消融术中的沉默肺静脉:意义和方法。","authors":"Peter Calvert, Wern Yew Ding, Michael Griffin, Arnaud Bisson, Ioanna Koniari, Noel Fitzpatrick, Richard Snowdon, Simon Modi, Vishal Luther, Saagar Mahida, Johan Waktare, Zoltan Borbas, Reza Ashrafi, Derick Todd, Dhiraj Gupta","doi":"10.1007/s10840-024-01750-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Pulmonary vein isolation (PVI) is the cornerstone of atrial fibrillation (AF) ablation. Despite promising success rates, redo ablation is sometimes required. At redo, PVs may be found to be isolated (silent) or reconnected. We studied patients with silent vs reconnected PVs at redo and analysed associations with adverse outcomes.</p><p><strong>Methods: </strong>Patients undergoing redo AF ablations between 2013 and 2019 at our institution were included and stratified into silent PVs or reconnected PVs. The primary outcome was a composite of further redo ablation, non-AF ablation, atrioventricular nodal ablation, and death. Secondary outcomes included arrhythmia recurrence.</p><p><strong>Results: </strong>A total of 467 patients were included with mean 4.6 ± 1.7 years follow-up, of whom 48 (10.3%) had silent PVs. The silent PV group had had more often undergone >1 prior ablation (45.8% vs 9.8%; p<0.001), had more persistent AF (62.5% vs 41.1%; p=0.005) and had more non-PV ablation performed both at prior ablation procedures and at the analysed redo ablation. The primary outcome occurred more frequently in those with silent PVs (25% vs 13.8%; p=0.053). Arrhythmia recurrence was also more common in the silent PV group (66.7% vs 50.6%; p=0.047). After multivariable adjustment, female sex (aHR 2.35 [95% CI 2.35-3.96]; p=0.001) and ischaemic heart disease (aHR 3.21 [95% CI 1.56-6.62]; p=0.002) were independently associated with the primary outcome, and left atrial enlargement (aHR 1.58 [95% CI 1.20-2.08]; p=0.001) and >1 prior ablation (aHR 1.88 [95% CI 1.30-2.72]; p<0.001) were independently associated with arrhythmia recurrence. Whilst a finding of silent PVs was not itself significant after multivariable adjustment, this provides an easily assessable parameter at clinically indicated redo ablation which informs the clinician of the likelihood of a worse future prognosis.</p><p><strong>Conclusions: </strong>Patients with silent PVs at redo AF ablation have worse clinical outcomes.</p>","PeriodicalId":16202,"journal":{"name":"Journal of Interventional Cardiac Electrophysiology","volume":null,"pages":null},"PeriodicalIF":2.1000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11289157/pdf/","citationCount":"0","resultStr":"{\"title\":\"Silent pulmonary veins at redo ablation for atrial fibrillation: Implications and approaches.\",\"authors\":\"Peter Calvert, Wern Yew Ding, Michael Griffin, Arnaud Bisson, Ioanna Koniari, Noel Fitzpatrick, Richard Snowdon, Simon Modi, Vishal Luther, Saagar Mahida, Johan Waktare, Zoltan Borbas, Reza Ashrafi, Derick Todd, Dhiraj Gupta\",\"doi\":\"10.1007/s10840-024-01750-w\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Pulmonary vein isolation (PVI) is the cornerstone of atrial fibrillation (AF) ablation. Despite promising success rates, redo ablation is sometimes required. At redo, PVs may be found to be isolated (silent) or reconnected. We studied patients with silent vs reconnected PVs at redo and analysed associations with adverse outcomes.</p><p><strong>Methods: </strong>Patients undergoing redo AF ablations between 2013 and 2019 at our institution were included and stratified into silent PVs or reconnected PVs. The primary outcome was a composite of further redo ablation, non-AF ablation, atrioventricular nodal ablation, and death. Secondary outcomes included arrhythmia recurrence.</p><p><strong>Results: </strong>A total of 467 patients were included with mean 4.6 ± 1.7 years follow-up, of whom 48 (10.3%) had silent PVs. The silent PV group had had more often undergone >1 prior ablation (45.8% vs 9.8%; p<0.001), had more persistent AF (62.5% vs 41.1%; p=0.005) and had more non-PV ablation performed both at prior ablation procedures and at the analysed redo ablation. The primary outcome occurred more frequently in those with silent PVs (25% vs 13.8%; p=0.053). Arrhythmia recurrence was also more common in the silent PV group (66.7% vs 50.6%; p=0.047). After multivariable adjustment, female sex (aHR 2.35 [95% CI 2.35-3.96]; p=0.001) and ischaemic heart disease (aHR 3.21 [95% CI 1.56-6.62]; p=0.002) were independently associated with the primary outcome, and left atrial enlargement (aHR 1.58 [95% CI 1.20-2.08]; p=0.001) and >1 prior ablation (aHR 1.88 [95% CI 1.30-2.72]; p<0.001) were independently associated with arrhythmia recurrence. Whilst a finding of silent PVs was not itself significant after multivariable adjustment, this provides an easily assessable parameter at clinically indicated redo ablation which informs the clinician of the likelihood of a worse future prognosis.</p><p><strong>Conclusions: </strong>Patients with silent PVs at redo AF ablation have worse clinical outcomes.</p>\",\"PeriodicalId\":16202,\"journal\":{\"name\":\"Journal of Interventional Cardiac Electrophysiology\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2024-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11289157/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Interventional Cardiac Electrophysiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s10840-024-01750-w\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/23 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Interventional Cardiac Electrophysiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10840-024-01750-w","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/23 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Silent pulmonary veins at redo ablation for atrial fibrillation: Implications and approaches.
Background: Pulmonary vein isolation (PVI) is the cornerstone of atrial fibrillation (AF) ablation. Despite promising success rates, redo ablation is sometimes required. At redo, PVs may be found to be isolated (silent) or reconnected. We studied patients with silent vs reconnected PVs at redo and analysed associations with adverse outcomes.
Methods: Patients undergoing redo AF ablations between 2013 and 2019 at our institution were included and stratified into silent PVs or reconnected PVs. The primary outcome was a composite of further redo ablation, non-AF ablation, atrioventricular nodal ablation, and death. Secondary outcomes included arrhythmia recurrence.
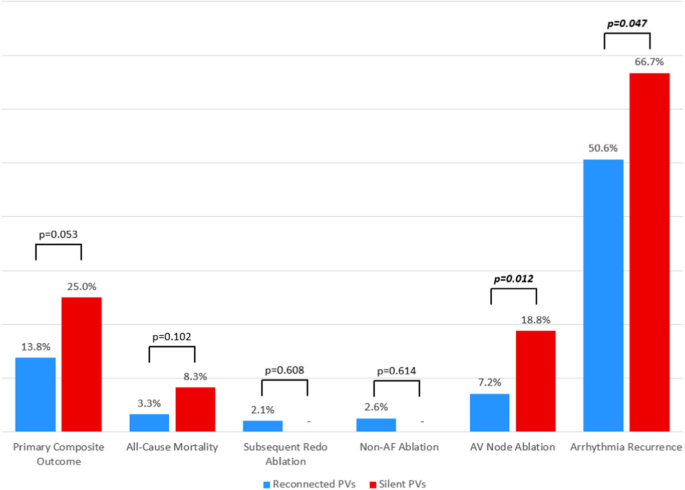
Results: A total of 467 patients were included with mean 4.6 ± 1.7 years follow-up, of whom 48 (10.3%) had silent PVs. The silent PV group had had more often undergone >1 prior ablation (45.8% vs 9.8%; p<0.001), had more persistent AF (62.5% vs 41.1%; p=0.005) and had more non-PV ablation performed both at prior ablation procedures and at the analysed redo ablation. The primary outcome occurred more frequently in those with silent PVs (25% vs 13.8%; p=0.053). Arrhythmia recurrence was also more common in the silent PV group (66.7% vs 50.6%; p=0.047). After multivariable adjustment, female sex (aHR 2.35 [95% CI 2.35-3.96]; p=0.001) and ischaemic heart disease (aHR 3.21 [95% CI 1.56-6.62]; p=0.002) were independently associated with the primary outcome, and left atrial enlargement (aHR 1.58 [95% CI 1.20-2.08]; p=0.001) and >1 prior ablation (aHR 1.88 [95% CI 1.30-2.72]; p<0.001) were independently associated with arrhythmia recurrence. Whilst a finding of silent PVs was not itself significant after multivariable adjustment, this provides an easily assessable parameter at clinically indicated redo ablation which informs the clinician of the likelihood of a worse future prognosis.
Conclusions: Patients with silent PVs at redo AF ablation have worse clinical outcomes.
期刊介绍:
The Journal of Interventional Cardiac Electrophysiology is an international publication devoted to fostering research in and development of interventional techniques and therapies for the management of cardiac arrhythmias. It is designed primarily to present original research studies and scholarly scientific reviews of basic and applied science and clinical research in this field. The Journal will adopt a multidisciplinary approach to link physical, experimental, and clinical sciences as applied to the development of and practice in interventional electrophysiology. The Journal will examine techniques ranging from molecular, chemical and pharmacologic therapies to device and ablation technology. Accordingly, original research in clinical, epidemiologic and basic science arenas will be considered for publication. Applied engineering or physical science studies pertaining to interventional electrophysiology will be encouraged. The Journal is committed to providing comprehensive and detailed treatment of major interventional therapies and innovative techniques in a structured and clinically relevant manner. It is directed at clinical practitioners and investigators in the rapidly growing field of interventional electrophysiology. The editorial staff and board reflect this bias and include noted international experts in this area with a wealth of expertise in basic and clinical investigation. Peer review of all submissions, conflict of interest guidelines and periodic editorial board review of all Journal policies have been established.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


