Andrew R Guillotte, Lane Fry, Domenico Gattozzi, Kushal Shah
{"title":"格拉斯哥昏迷量表运动评分预测创伤性脑损伤减压颅骨切除术后气管造口术的必要性。","authors":"Andrew R Guillotte, Lane Fry, Domenico Gattozzi, Kushal Shah","doi":"10.13004/kjnt.2023.19.e53","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Many patients with severe traumatic brain injury (TBI) require a tracheostomy after decompressive craniectomy. Determining which patients will require tracheostomy is often challenging. The existing methods for predicting which patients will require tracheostomy are more applicable to stroke and spontaneous intracranial hemorrhage. The aim of this study was to investigate whether the Glasgow Coma Scale (GCS) motor score can be used as a screening method for predicting which patients who undergo decompressive craniectomy for severe TBI are likely to require tracheostomy.</p><p><strong>Methods: </strong>The neurosurgery census at the University of Kansas Medical Center was retrospectively reviewed to identify adult patients aged over 18 years who underwent decompressive craniectomy for TBI. Eighty patients met the inclusion criteria for the study. There were no exclusion criteria. The primary outcome of interest was the need for tracheostomy. The secondary outcome was the comparison of the total length of stay (LOS) and intensive care unit LOS between the early and late tracheostomy patient groups.</p><p><strong>Results: </strong>All patients (100%) with a GCS motor score of 4 or less on post operative (POD) 5 required tracheostomy. Setting the threshold at GCS motor score of 5 on POD 5 for recommending tracheostomy resulted in 86.7% sensitivity, 91.7% specificity, and 90.5% positive predictive value, with an area under the receiver operator curve of 0.9101.</p><p><strong>Conclusion: </strong>GCS motor score of 5 or less on POD 5 of decompressive craniectomy is a useful screening threshold for selecting patients who may benefit from tracheostomy, or may be potential candidates for extubation.</p>","PeriodicalId":36879,"journal":{"name":"Korean Journal of Neurotrauma","volume":"19 4","pages":"454-465"},"PeriodicalIF":0.0000,"publicationDate":"2023-11-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10782100/pdf/","citationCount":"0","resultStr":"{\"title\":\"Glasgow Coma Scale Motor Score Predicts Need for Tracheostomy After Decompressive Craniectomy for Traumatic Brain Injury.\",\"authors\":\"Andrew R Guillotte, Lane Fry, Domenico Gattozzi, Kushal Shah\",\"doi\":\"10.13004/kjnt.2023.19.e53\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>Many patients with severe traumatic brain injury (TBI) require a tracheostomy after decompressive craniectomy. Determining which patients will require tracheostomy is often challenging. The existing methods for predicting which patients will require tracheostomy are more applicable to stroke and spontaneous intracranial hemorrhage. The aim of this study was to investigate whether the Glasgow Coma Scale (GCS) motor score can be used as a screening method for predicting which patients who undergo decompressive craniectomy for severe TBI are likely to require tracheostomy.</p><p><strong>Methods: </strong>The neurosurgery census at the University of Kansas Medical Center was retrospectively reviewed to identify adult patients aged over 18 years who underwent decompressive craniectomy for TBI. Eighty patients met the inclusion criteria for the study. There were no exclusion criteria. The primary outcome of interest was the need for tracheostomy. The secondary outcome was the comparison of the total length of stay (LOS) and intensive care unit LOS between the early and late tracheostomy patient groups.</p><p><strong>Results: </strong>All patients (100%) with a GCS motor score of 4 or less on post operative (POD) 5 required tracheostomy. Setting the threshold at GCS motor score of 5 on POD 5 for recommending tracheostomy resulted in 86.7% sensitivity, 91.7% specificity, and 90.5% positive predictive value, with an area under the receiver operator curve of 0.9101.</p><p><strong>Conclusion: </strong>GCS motor score of 5 or less on POD 5 of decompressive craniectomy is a useful screening threshold for selecting patients who may benefit from tracheostomy, or may be potential candidates for extubation.</p>\",\"PeriodicalId\":36879,\"journal\":{\"name\":\"Korean Journal of Neurotrauma\",\"volume\":\"19 4\",\"pages\":\"454-465\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-11-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10782100/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Korean Journal of Neurotrauma\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.13004/kjnt.2023.19.e53\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/12/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Korean Journal of Neurotrauma","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.13004/kjnt.2023.19.e53","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/12/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
Glasgow Coma Scale Motor Score Predicts Need for Tracheostomy After Decompressive Craniectomy for Traumatic Brain Injury.
Objective: Many patients with severe traumatic brain injury (TBI) require a tracheostomy after decompressive craniectomy. Determining which patients will require tracheostomy is often challenging. The existing methods for predicting which patients will require tracheostomy are more applicable to stroke and spontaneous intracranial hemorrhage. The aim of this study was to investigate whether the Glasgow Coma Scale (GCS) motor score can be used as a screening method for predicting which patients who undergo decompressive craniectomy for severe TBI are likely to require tracheostomy.
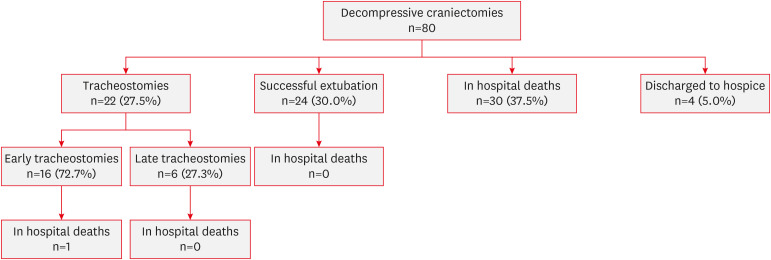
Methods: The neurosurgery census at the University of Kansas Medical Center was retrospectively reviewed to identify adult patients aged over 18 years who underwent decompressive craniectomy for TBI. Eighty patients met the inclusion criteria for the study. There were no exclusion criteria. The primary outcome of interest was the need for tracheostomy. The secondary outcome was the comparison of the total length of stay (LOS) and intensive care unit LOS between the early and late tracheostomy patient groups.
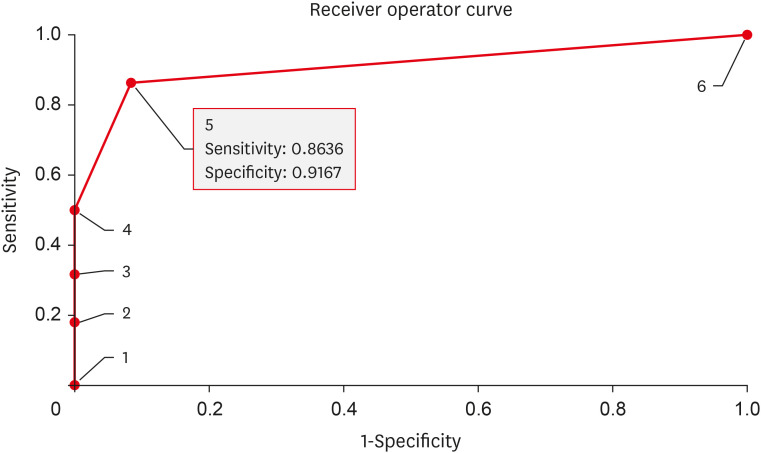
Results: All patients (100%) with a GCS motor score of 4 or less on post operative (POD) 5 required tracheostomy. Setting the threshold at GCS motor score of 5 on POD 5 for recommending tracheostomy resulted in 86.7% sensitivity, 91.7% specificity, and 90.5% positive predictive value, with an area under the receiver operator curve of 0.9101.
Conclusion: GCS motor score of 5 or less on POD 5 of decompressive craniectomy is a useful screening threshold for selecting patients who may benefit from tracheostomy, or may be potential candidates for extubation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


