Jorge Jorquera, Jorge Dreyse, Constanza Salas, Francisca Letelier, Bunio Weissglas, Javiera Del-Río, Mario Henríquez-Beltrán, Gonzalo Labarca, Jorge Jorquera-Díaz
{"title":"睡眠呼吸暂停多组分分级系统的临床应用与心血管死亡率事件。","authors":"Jorge Jorquera, Jorge Dreyse, Constanza Salas, Francisca Letelier, Bunio Weissglas, Javiera Del-Río, Mario Henríquez-Beltrán, Gonzalo Labarca, Jorge Jorquera-Díaz","doi":"10.1055/s-0043-1776770","DOIUrl":null,"url":null,"abstract":"<p><p><b>Objective</b> To evaluate the clinical utility of the Baveno classification in predicting incident cardiovascular mortality after five years of follow-up in a clinic-based cohort of patients with obstructive sleep apnea (OSA). <b>Materials and Methods</b> We evaluated the reproducibility of the Baveno classification using data from the Santiago Obstructive Sleep Apnea (SantOSA) study. The groups were labeled Baveno A (minor symptoms and comorbidities), B (severe symptoms and minor comorbidities), C (minor symptoms and severe comorbidities), and D (severe symptoms and comorbidities). Within-group comparisons were performed using analysis of variance (ANOVA) and post hoc tests. The associations between groups and incident cardiovascular mortality were determined through the Mantel-Cox and Cox proportional hazard ratios (HRs) adjusted by covariables. <b>Results</b> A total of 1,300 OSA patients were included (Baveno A: 27.7%; B: 28%; C: 16.8%; and D: 27.5%). The follow-up was of 5.4 years. Compared to Baveno A, the fully-adjusted risk of cardiovascular mortality with Baveno B presented an HR of 1.38 (95% confidence interval [95%CI]: 0.14-13.5; <i>p</i> = 0.78); with Baveno C, it was of 1.71 (95%CI: 0.18-16.2; <i>p</i> = 0.63); and, with Baveno D, of 1.04 (95%CI: 0.12-9.2; <i>p</i> = 0.98). We found no interactions involving Baveno group, sex and OSA severity. <b>Discussion</b> Among OSA patients, the Baveno classification can describe different subgroups. However, its utility in identifying incident cardiovascular mortality is unclear. Long-term follow-up studies and the inclusion of demographic variables in the classification could improve its ability to detect a high-risk phenotype associated with cardiovascular mortality. <b>Conclusion</b> The Baveno classification serves as a valuable method for categorizing varying groups of patients afflicted with OSA. Nevertheless, its precision in identifying occurrence of cardiovascular mortality is still unclear.</p>","PeriodicalId":21848,"journal":{"name":"Sleep Science","volume":"16 4","pages":"e446-e453"},"PeriodicalIF":1.8000,"publicationDate":"2023-11-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10773515/pdf/","citationCount":"0","resultStr":"{\"title\":\"Clinical Application of the Multicomponent Grading System for Sleep Apnea Classification and Incident Cardiovascular Mortality.\",\"authors\":\"Jorge Jorquera, Jorge Dreyse, Constanza Salas, Francisca Letelier, Bunio Weissglas, Javiera Del-Río, Mario Henríquez-Beltrán, Gonzalo Labarca, Jorge Jorquera-Díaz\",\"doi\":\"10.1055/s-0043-1776770\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Objective</b> To evaluate the clinical utility of the Baveno classification in predicting incident cardiovascular mortality after five years of follow-up in a clinic-based cohort of patients with obstructive sleep apnea (OSA). <b>Materials and Methods</b> We evaluated the reproducibility of the Baveno classification using data from the Santiago Obstructive Sleep Apnea (SantOSA) study. The groups were labeled Baveno A (minor symptoms and comorbidities), B (severe symptoms and minor comorbidities), C (minor symptoms and severe comorbidities), and D (severe symptoms and comorbidities). Within-group comparisons were performed using analysis of variance (ANOVA) and post hoc tests. The associations between groups and incident cardiovascular mortality were determined through the Mantel-Cox and Cox proportional hazard ratios (HRs) adjusted by covariables. <b>Results</b> A total of 1,300 OSA patients were included (Baveno A: 27.7%; B: 28%; C: 16.8%; and D: 27.5%). The follow-up was of 5.4 years. Compared to Baveno A, the fully-adjusted risk of cardiovascular mortality with Baveno B presented an HR of 1.38 (95% confidence interval [95%CI]: 0.14-13.5; <i>p</i> = 0.78); with Baveno C, it was of 1.71 (95%CI: 0.18-16.2; <i>p</i> = 0.63); and, with Baveno D, of 1.04 (95%CI: 0.12-9.2; <i>p</i> = 0.98). We found no interactions involving Baveno group, sex and OSA severity. <b>Discussion</b> Among OSA patients, the Baveno classification can describe different subgroups. However, its utility in identifying incident cardiovascular mortality is unclear. Long-term follow-up studies and the inclusion of demographic variables in the classification could improve its ability to detect a high-risk phenotype associated with cardiovascular mortality. <b>Conclusion</b> The Baveno classification serves as a valuable method for categorizing varying groups of patients afflicted with OSA. Nevertheless, its precision in identifying occurrence of cardiovascular mortality is still unclear.</p>\",\"PeriodicalId\":21848,\"journal\":{\"name\":\"Sleep Science\",\"volume\":\"16 4\",\"pages\":\"e446-e453\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2023-11-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10773515/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Sleep Science\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1055/s-0043-1776770\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/12/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Sleep Science","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0043-1776770","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/12/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
目的 评估阻塞性睡眠呼吸暂停(OSA)患者临床队列随访五年后,巴韦诺分类法在预测心血管疾病死亡率方面的临床实用性。材料与方法 我们利用圣地亚哥阻塞性睡眠呼吸暂停(SantOSA)研究的数据评估了巴韦诺分类法的可重复性。各组分别标记为巴韦诺 A 组(轻微症状和合并症)、B 组(严重症状和轻微合并症)、C 组(轻微症状和严重合并症)和 D 组(严重症状和合并症)。组内比较采用方差分析(ANOVA)和事后检验。各组与心血管疾病死亡率之间的关系通过经协变量调整的 Mantel-Cox 和 Cox 比例危险比 (HRs) 来确定。结果 共纳入 1300 名 OSA 患者(Baveno A:27.7%;B:28%;C:16.8%;D:27.5%)。随访时间为 5.4 年。与贝文诺 A 相比,贝文诺 B 的完全调整后心血管死亡风险 HR 为 1.38(95% 置信区间 [95%CI]:0.14-13.5;p = 0.78);贝文诺 C 为 1.71(95%CI:0.18-16.2;p = 0.63);贝文诺 D 为 1.04(95%CI:0.12-9.2;p = 0.98)。我们没有发现贝文诺组别、性别和 OSA 严重程度之间存在相互作用。讨论 在 OSA 患者中,巴韦诺分类可以描述不同的亚组。然而,其在确定心血管疾病死亡率方面的作用尚不明确。长期随访研究以及在分类中加入人口统计学变量可提高其检测与心血管死亡相关的高风险表型的能力。结论 巴韦诺分类法是对不同OSA患者群体进行分类的重要方法。然而,它在识别心血管死亡发生方面的准确性仍不明确。
Clinical Application of the Multicomponent Grading System for Sleep Apnea Classification and Incident Cardiovascular Mortality.
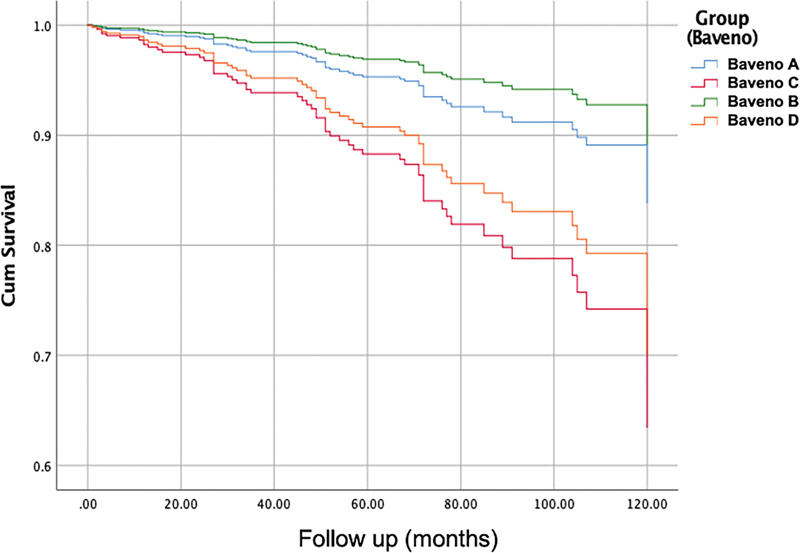
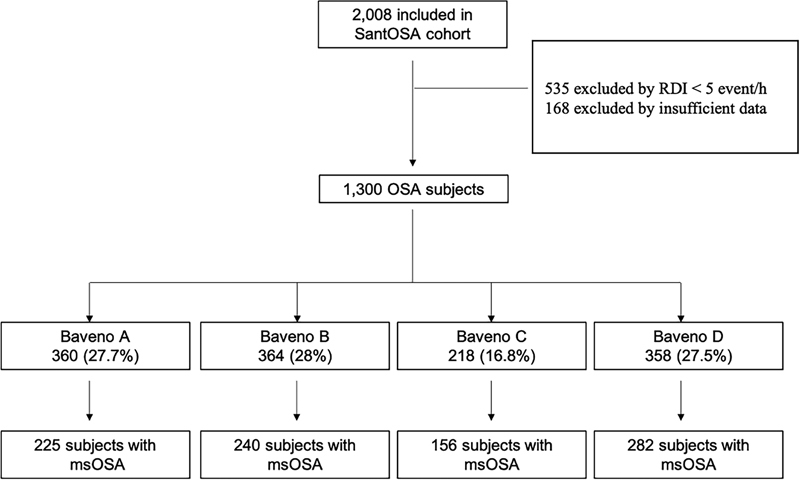
Objective To evaluate the clinical utility of the Baveno classification in predicting incident cardiovascular mortality after five years of follow-up in a clinic-based cohort of patients with obstructive sleep apnea (OSA). Materials and Methods We evaluated the reproducibility of the Baveno classification using data from the Santiago Obstructive Sleep Apnea (SantOSA) study. The groups were labeled Baveno A (minor symptoms and comorbidities), B (severe symptoms and minor comorbidities), C (minor symptoms and severe comorbidities), and D (severe symptoms and comorbidities). Within-group comparisons were performed using analysis of variance (ANOVA) and post hoc tests. The associations between groups and incident cardiovascular mortality were determined through the Mantel-Cox and Cox proportional hazard ratios (HRs) adjusted by covariables. Results A total of 1,300 OSA patients were included (Baveno A: 27.7%; B: 28%; C: 16.8%; and D: 27.5%). The follow-up was of 5.4 years. Compared to Baveno A, the fully-adjusted risk of cardiovascular mortality with Baveno B presented an HR of 1.38 (95% confidence interval [95%CI]: 0.14-13.5; p = 0.78); with Baveno C, it was of 1.71 (95%CI: 0.18-16.2; p = 0.63); and, with Baveno D, of 1.04 (95%CI: 0.12-9.2; p = 0.98). We found no interactions involving Baveno group, sex and OSA severity. Discussion Among OSA patients, the Baveno classification can describe different subgroups. However, its utility in identifying incident cardiovascular mortality is unclear. Long-term follow-up studies and the inclusion of demographic variables in the classification could improve its ability to detect a high-risk phenotype associated with cardiovascular mortality. Conclusion The Baveno classification serves as a valuable method for categorizing varying groups of patients afflicted with OSA. Nevertheless, its precision in identifying occurrence of cardiovascular mortality is still unclear.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


