Nabeel Mansour, Simon Sirtl, Martin K Angele, Moritz Wildgruber
{"title":"胰十二指肠切除术后窦状门脉高压的处理方法","authors":"Nabeel Mansour, Simon Sirtl, Martin K Angele, Moritz Wildgruber","doi":"10.1159/000535774","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Sinistral, or left-sided, portal hypertension (SPH) is a rare cause of upper gastrointestinal (GI) hemorrhage resulting from obstruction of the splenic vein. Venous drainage from the spleen via collaterals can result in venous hemorrhage into both the retroperitoneal and intra-abdominal spaces due to increased venous blood pressure in peripancreatic and gastroduodenal vasculature. SPH can occur secondary to pancreatitis with thrombosis of the splenic vein. Another possible cause is the surgical ligation of the splenic vein as part of pancreaticoduodenectomy (PD). Although splenectomy has been traditionally considered as the treatment of choice to relieve venous hypertension, individual concepts for each patient have to be developed. Considering the venous collateral drainage pathways, a comprehensive approach involving surgical, endoscopic, and interventional radiology interventions may be necessary to address the underlying cause of variceal bleeding. Among these approaches, splenic artery embolization (SAE) has demonstrated efficacy in mitigating the adverse effects associated with elevated venous outflow pressure.</p><p><strong>Summary: </strong>This review summarizes key imaging findings in SPH patients after PD and highlights the potential of minimally invasive embolization for curative treatment of variceal hemorrhage.</p><p><strong>Key messages: </strong>(i) SPH is a potential consequence after major pancreas surgery. (ii) Collateral flow can lead to life-threatening abdominal bleeding. (iii) Depending on the origin and localization of the bleeding, a dedicated management is required, frequently involving interventional radiology techniques.</p>","PeriodicalId":11294,"journal":{"name":"Digestive Diseases","volume":" ","pages":"178-185"},"PeriodicalIF":2.1000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10997249/pdf/","citationCount":"0","resultStr":"{\"title\":\"Management of Sinistral Portal Hypertension after Pancreaticoduodenectomy.\",\"authors\":\"Nabeel Mansour, Simon Sirtl, Martin K Angele, Moritz Wildgruber\",\"doi\":\"10.1159/000535774\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Sinistral, or left-sided, portal hypertension (SPH) is a rare cause of upper gastrointestinal (GI) hemorrhage resulting from obstruction of the splenic vein. Venous drainage from the spleen via collaterals can result in venous hemorrhage into both the retroperitoneal and intra-abdominal spaces due to increased venous blood pressure in peripancreatic and gastroduodenal vasculature. SPH can occur secondary to pancreatitis with thrombosis of the splenic vein. Another possible cause is the surgical ligation of the splenic vein as part of pancreaticoduodenectomy (PD). Although splenectomy has been traditionally considered as the treatment of choice to relieve venous hypertension, individual concepts for each patient have to be developed. Considering the venous collateral drainage pathways, a comprehensive approach involving surgical, endoscopic, and interventional radiology interventions may be necessary to address the underlying cause of variceal bleeding. Among these approaches, splenic artery embolization (SAE) has demonstrated efficacy in mitigating the adverse effects associated with elevated venous outflow pressure.</p><p><strong>Summary: </strong>This review summarizes key imaging findings in SPH patients after PD and highlights the potential of minimally invasive embolization for curative treatment of variceal hemorrhage.</p><p><strong>Key messages: </strong>(i) SPH is a potential consequence after major pancreas surgery. (ii) Collateral flow can lead to life-threatening abdominal bleeding. (iii) Depending on the origin and localization of the bleeding, a dedicated management is required, frequently involving interventional radiology techniques.</p>\",\"PeriodicalId\":11294,\"journal\":{\"name\":\"Digestive Diseases\",\"volume\":\" \",\"pages\":\"178-185\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2024-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10997249/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Digestive Diseases\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1159/000535774\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/5 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Digestive Diseases","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1159/000535774","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/5 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Management of Sinistral Portal Hypertension after Pancreaticoduodenectomy.
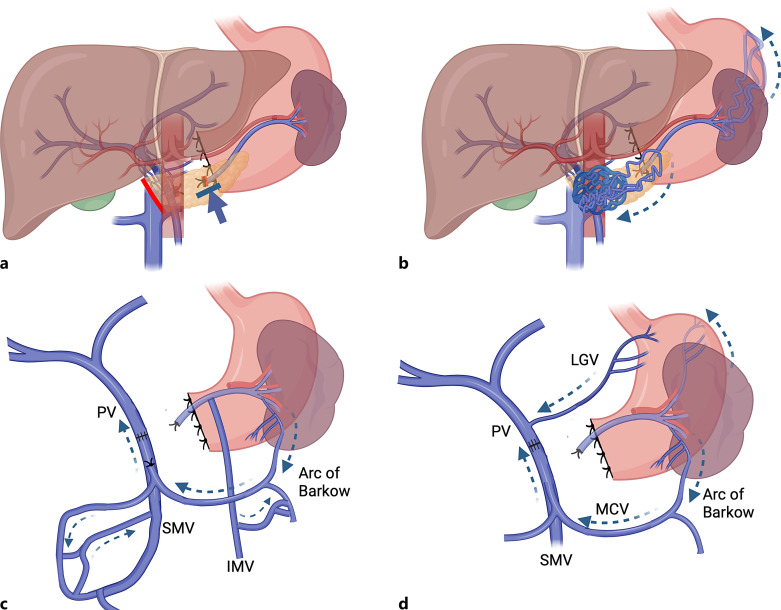
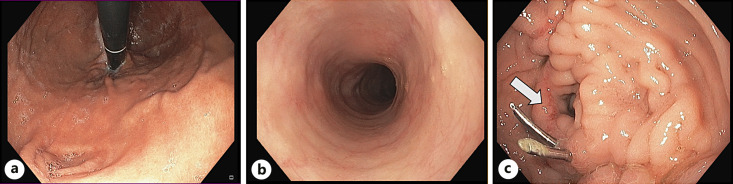
Background: Sinistral, or left-sided, portal hypertension (SPH) is a rare cause of upper gastrointestinal (GI) hemorrhage resulting from obstruction of the splenic vein. Venous drainage from the spleen via collaterals can result in venous hemorrhage into both the retroperitoneal and intra-abdominal spaces due to increased venous blood pressure in peripancreatic and gastroduodenal vasculature. SPH can occur secondary to pancreatitis with thrombosis of the splenic vein. Another possible cause is the surgical ligation of the splenic vein as part of pancreaticoduodenectomy (PD). Although splenectomy has been traditionally considered as the treatment of choice to relieve venous hypertension, individual concepts for each patient have to be developed. Considering the venous collateral drainage pathways, a comprehensive approach involving surgical, endoscopic, and interventional radiology interventions may be necessary to address the underlying cause of variceal bleeding. Among these approaches, splenic artery embolization (SAE) has demonstrated efficacy in mitigating the adverse effects associated with elevated venous outflow pressure.
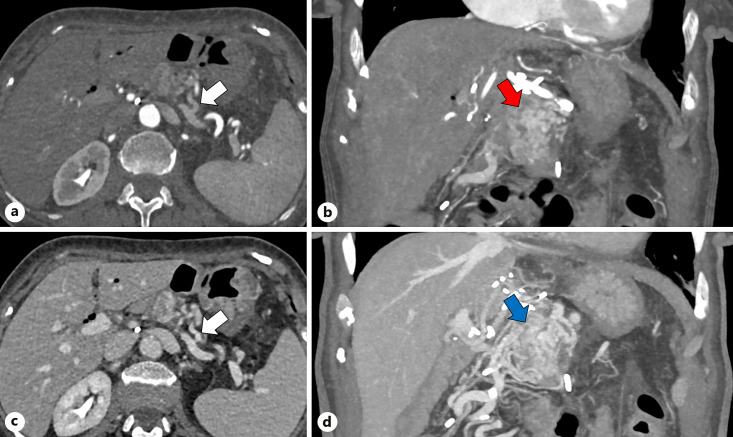
Summary: This review summarizes key imaging findings in SPH patients after PD and highlights the potential of minimally invasive embolization for curative treatment of variceal hemorrhage.
Key messages: (i) SPH is a potential consequence after major pancreas surgery. (ii) Collateral flow can lead to life-threatening abdominal bleeding. (iii) Depending on the origin and localization of the bleeding, a dedicated management is required, frequently involving interventional radiology techniques.
期刊介绍:
Each issue of this journal is dedicated to a special topic of current interest, covering both clinical and basic science topics in gastrointestinal function and disorders. The contents of each issue are comprehensive and reflect the state of the art, featuring editorials, reviews, mini reviews and original papers. These individual contributions encompass a variety of disciplines including all fields of gastroenterology. ''Digestive Diseases'' bridges the communication gap between advances made in the academic setting and their application in patient care. The journal is a valuable service for clinicians, specialists and physicians-in-training.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


