{"title":"预测未侵犯大弯的上部晚期胃癌脾门结节转移的关键结节站","authors":"Masashi Nishino, Takaki Yoshikawa, Masahiro Yura, Rei Ogawa, Ryota Sakon, Kenichi Ishizu, Takeyuki Wada, Tsutomu Hayashi, Yukinori Yamagata","doi":"10.1002/ags3.12759","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Standard surgery for upper advanced gastric cancer without invasion of the greater curvature (UGC-GC) is spleen-preserving D2 total gastrectomy without dissection of the splenic-hilar nodes (#10). However, some patients with nodal metastasis to #10 survive more than 5 years due to nodal dissection of #10. If nodal metastasis to #10 is predictable based on the positivity of other nodes dissected by the current standard surgery without #10 nodal dissection, physicians may be able to consider #10 dissection.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>This study retrospectively reviewed data from the National Cancer Center Hospital in Japan between 2000 and 2012. We selected cases that met the following criteria: (1) D2 or more total gastrectomy with splenectomy, (2) UGC-GC, and (3) histological type is gastric adenocarcinoma. We performed univariate and multivariate analyses concerning lymph node stations associated with #10 metastasis.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>A total of 366 patients were examined. A multivariate analysis revealed that #10 metastasis was associated with positivity of the nodes along the short gastric arteries (#4sa) and distal nodes along the splenic artery (#11d) (#4sa: <i>p</i> = 0.003, #11d: <i>p</i> = 0.016). When either key node was positive, the metastatic rate of #10 was 24.4%, and the therapeutic value index was 13.3.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>#4sa and #11d were key lymph nodes predicting #10 nodal metastasis in UGC-GC. When these key nodes are positive on computed tomography before surgery or according to a rapid pathological examination during surgery, dissection of #10 should be considered even if upper advanced tumors are not invading the greater curvature.</p>\n </section>\n </div>","PeriodicalId":8030,"journal":{"name":"Annals of Gastroenterological Surgery","volume":"8 3","pages":"413-419"},"PeriodicalIF":3.3000,"publicationDate":"2023-11-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ags3.12759","citationCount":"0","resultStr":"{\"title\":\"Key nodal stations for predicting splenic hilar nodal metastasis in upper advanced gastric cancer without invasion of the greater curvature\",\"authors\":\"Masashi Nishino, Takaki Yoshikawa, Masahiro Yura, Rei Ogawa, Ryota Sakon, Kenichi Ishizu, Takeyuki Wada, Tsutomu Hayashi, Yukinori Yamagata\",\"doi\":\"10.1002/ags3.12759\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Standard surgery for upper advanced gastric cancer without invasion of the greater curvature (UGC-GC) is spleen-preserving D2 total gastrectomy without dissection of the splenic-hilar nodes (#10). However, some patients with nodal metastasis to #10 survive more than 5 years due to nodal dissection of #10. If nodal metastasis to #10 is predictable based on the positivity of other nodes dissected by the current standard surgery without #10 nodal dissection, physicians may be able to consider #10 dissection.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>This study retrospectively reviewed data from the National Cancer Center Hospital in Japan between 2000 and 2012. We selected cases that met the following criteria: (1) D2 or more total gastrectomy with splenectomy, (2) UGC-GC, and (3) histological type is gastric adenocarcinoma. We performed univariate and multivariate analyses concerning lymph node stations associated with #10 metastasis.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>A total of 366 patients were examined. A multivariate analysis revealed that #10 metastasis was associated with positivity of the nodes along the short gastric arteries (#4sa) and distal nodes along the splenic artery (#11d) (#4sa: <i>p</i> = 0.003, #11d: <i>p</i> = 0.016). When either key node was positive, the metastatic rate of #10 was 24.4%, and the therapeutic value index was 13.3.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>#4sa and #11d were key lymph nodes predicting #10 nodal metastasis in UGC-GC. When these key nodes are positive on computed tomography before surgery or according to a rapid pathological examination during surgery, dissection of #10 should be considered even if upper advanced tumors are not invading the greater curvature.</p>\\n </section>\\n </div>\",\"PeriodicalId\":8030,\"journal\":{\"name\":\"Annals of Gastroenterological Surgery\",\"volume\":\"8 3\",\"pages\":\"413-419\"},\"PeriodicalIF\":3.3000,\"publicationDate\":\"2023-11-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ags3.12759\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Gastroenterological Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ags3.12759\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Gastroenterological Surgery","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ags3.12759","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Key nodal stations for predicting splenic hilar nodal metastasis in upper advanced gastric cancer without invasion of the greater curvature
Background
Standard surgery for upper advanced gastric cancer without invasion of the greater curvature (UGC-GC) is spleen-preserving D2 total gastrectomy without dissection of the splenic-hilar nodes (#10). However, some patients with nodal metastasis to #10 survive more than 5 years due to nodal dissection of #10. If nodal metastasis to #10 is predictable based on the positivity of other nodes dissected by the current standard surgery without #10 nodal dissection, physicians may be able to consider #10 dissection.
Methods
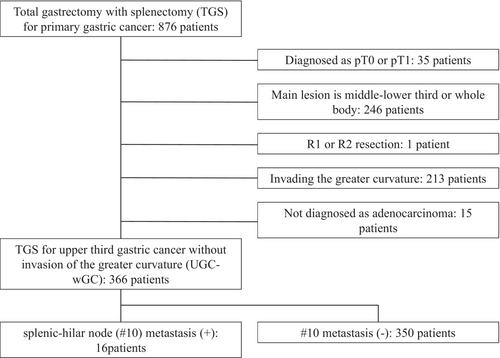
This study retrospectively reviewed data from the National Cancer Center Hospital in Japan between 2000 and 2012. We selected cases that met the following criteria: (1) D2 or more total gastrectomy with splenectomy, (2) UGC-GC, and (3) histological type is gastric adenocarcinoma. We performed univariate and multivariate analyses concerning lymph node stations associated with #10 metastasis.
Results
A total of 366 patients were examined. A multivariate analysis revealed that #10 metastasis was associated with positivity of the nodes along the short gastric arteries (#4sa) and distal nodes along the splenic artery (#11d) (#4sa: p = 0.003, #11d: p = 0.016). When either key node was positive, the metastatic rate of #10 was 24.4%, and the therapeutic value index was 13.3.
Conclusions
#4sa and #11d were key lymph nodes predicting #10 nodal metastasis in UGC-GC. When these key nodes are positive on computed tomography before surgery or according to a rapid pathological examination during surgery, dissection of #10 should be considered even if upper advanced tumors are not invading the greater curvature.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


