Alice Piccato MD, Alessandro Crosio MD, Andrea Antonini MD, Bruno Battiston MD, PhD, Paolo Titolo MD, Pierluigi Tos MD, PhD, Davide Ciclamini MD
{"title":"慢性骨髓炎的单阶段骨瓣重建与两阶段骨瓣重建:多中心结果比较","authors":"Alice Piccato MD, Alessandro Crosio MD, Andrea Antonini MD, Bruno Battiston MD, PhD, Paolo Titolo MD, Pierluigi Tos MD, PhD, Davide Ciclamini MD","doi":"10.1002/micr.31139","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Chronic osteomyelitis is an invalidating disease, and its severity grows according to the infection's particular features. The Cierny-Maiden criteria classify it according to the anatomical aspects (I to IV) and also by physiological class (A host being in good immune condition and B hosts being locally (L) or systemically (S) compromised). The surgical approach to chronic osteomyelitis involves radical debridement and dead space reconstruction. Two-stage management with delayed reconstruction is the most common surgical management, while one-stage treatment with concomitant reconstruction is a more aggressive approach with less available literature. Which method gives the best results is unclear. The purpose of this study is to compare single and two-stage techniques.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>The authors carried out a retrospective multicentric cohort study to compare two primary outcomes (bone union and infection healing) in one versus two-stage reconstructions with vascularized bone flaps in 23 cases of limb osteomyelitis (22 patients, 23 extremities). Thirteen subjects (56.5%) sustained a single-stage treatment consisting of a single surgery of radical debridement, concomitant soft tissue coverage, and bone reconstruction. Ten cases (43.5%) sustained a two-stage approach: radical debridement, simultaneous primary soft tissue closure, and antibiotic PMMA spacers implanted in 7 patients.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>No statistical differences were observed between one- and two-stage approaches in bone union rate and infection recurrence risk. Even though bone union seems to be higher and faster in the two-stage than in the one-stage group, and all infection relapses occurred in the one-stage group, data did not statistically confirm these differences. Two of the six cases (33.3%) of bone nonunion occurred in compromised hosts (representing only 17.4% of our sample). The B-hosts bone union rate was 50.0%, while it reached 78.9% in A-hosts, but the difference was not statistically significant (<i>p</i> = .5392). Infection recurrence was higher in B-hosts than in A-hosts (<i>p</i> = .0086) and in <i>Pseudomonas aeruginosa</i> sustained infections (<i>p</i> = .0208), but in the latter case, the treatment strategy did not influence the outcome (<i>p</i> = .4000).</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Bone union and infection healing rates are comparable between one and two-stage approaches. <i>Pseudomonas aeruginosa</i> infections have a higher risk of infection relapse, with similar effectiveness of one- and two-stage strategies. B-hosts have a higher infection recurrence rate without comparable data between the two approaches. Further studies with a larger sample size are required to confirm our results and define B-hosts' best strategy.</p>\n </section>\n \n <section>\n \n <h3> Level of Evidence</h3>\n \n <p>Level III of evidence, retrospective cohort study investigating the results of treatments.</p>\n </section>\n </div>","PeriodicalId":18600,"journal":{"name":"Microsurgery","volume":"44 1","pages":""},"PeriodicalIF":1.7000,"publicationDate":"2023-12-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/micr.31139","citationCount":"0","resultStr":"{\"title\":\"Single-stage versus two-stage bone flap reconstruction in chronic osteomyelitis: Multicenter outcomes comparison\",\"authors\":\"Alice Piccato MD, Alessandro Crosio MD, Andrea Antonini MD, Bruno Battiston MD, PhD, Paolo Titolo MD, Pierluigi Tos MD, PhD, Davide Ciclamini MD\",\"doi\":\"10.1002/micr.31139\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Chronic osteomyelitis is an invalidating disease, and its severity grows according to the infection's particular features. The Cierny-Maiden criteria classify it according to the anatomical aspects (I to IV) and also by physiological class (A host being in good immune condition and B hosts being locally (L) or systemically (S) compromised). The surgical approach to chronic osteomyelitis involves radical debridement and dead space reconstruction. Two-stage management with delayed reconstruction is the most common surgical management, while one-stage treatment with concomitant reconstruction is a more aggressive approach with less available literature. Which method gives the best results is unclear. The purpose of this study is to compare single and two-stage techniques.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>The authors carried out a retrospective multicentric cohort study to compare two primary outcomes (bone union and infection healing) in one versus two-stage reconstructions with vascularized bone flaps in 23 cases of limb osteomyelitis (22 patients, 23 extremities). Thirteen subjects (56.5%) sustained a single-stage treatment consisting of a single surgery of radical debridement, concomitant soft tissue coverage, and bone reconstruction. Ten cases (43.5%) sustained a two-stage approach: radical debridement, simultaneous primary soft tissue closure, and antibiotic PMMA spacers implanted in 7 patients.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>No statistical differences were observed between one- and two-stage approaches in bone union rate and infection recurrence risk. Even though bone union seems to be higher and faster in the two-stage than in the one-stage group, and all infection relapses occurred in the one-stage group, data did not statistically confirm these differences. Two of the six cases (33.3%) of bone nonunion occurred in compromised hosts (representing only 17.4% of our sample). The B-hosts bone union rate was 50.0%, while it reached 78.9% in A-hosts, but the difference was not statistically significant (<i>p</i> = .5392). Infection recurrence was higher in B-hosts than in A-hosts (<i>p</i> = .0086) and in <i>Pseudomonas aeruginosa</i> sustained infections (<i>p</i> = .0208), but in the latter case, the treatment strategy did not influence the outcome (<i>p</i> = .4000).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>Bone union and infection healing rates are comparable between one and two-stage approaches. <i>Pseudomonas aeruginosa</i> infections have a higher risk of infection relapse, with similar effectiveness of one- and two-stage strategies. B-hosts have a higher infection recurrence rate without comparable data between the two approaches. Further studies with a larger sample size are required to confirm our results and define B-hosts' best strategy.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Level of Evidence</h3>\\n \\n <p>Level III of evidence, retrospective cohort study investigating the results of treatments.</p>\\n </section>\\n </div>\",\"PeriodicalId\":18600,\"journal\":{\"name\":\"Microsurgery\",\"volume\":\"44 1\",\"pages\":\"\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2023-12-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/micr.31139\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Microsurgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/micr.31139\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Microsurgery","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/micr.31139","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
Single-stage versus two-stage bone flap reconstruction in chronic osteomyelitis: Multicenter outcomes comparison
Background
Chronic osteomyelitis is an invalidating disease, and its severity grows according to the infection's particular features. The Cierny-Maiden criteria classify it according to the anatomical aspects (I to IV) and also by physiological class (A host being in good immune condition and B hosts being locally (L) or systemically (S) compromised). The surgical approach to chronic osteomyelitis involves radical debridement and dead space reconstruction. Two-stage management with delayed reconstruction is the most common surgical management, while one-stage treatment with concomitant reconstruction is a more aggressive approach with less available literature. Which method gives the best results is unclear. The purpose of this study is to compare single and two-stage techniques.
Methods
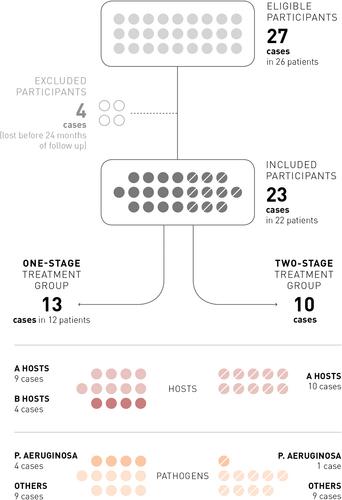
The authors carried out a retrospective multicentric cohort study to compare two primary outcomes (bone union and infection healing) in one versus two-stage reconstructions with vascularized bone flaps in 23 cases of limb osteomyelitis (22 patients, 23 extremities). Thirteen subjects (56.5%) sustained a single-stage treatment consisting of a single surgery of radical debridement, concomitant soft tissue coverage, and bone reconstruction. Ten cases (43.5%) sustained a two-stage approach: radical debridement, simultaneous primary soft tissue closure, and antibiotic PMMA spacers implanted in 7 patients.
Results
No statistical differences were observed between one- and two-stage approaches in bone union rate and infection recurrence risk. Even though bone union seems to be higher and faster in the two-stage than in the one-stage group, and all infection relapses occurred in the one-stage group, data did not statistically confirm these differences. Two of the six cases (33.3%) of bone nonunion occurred in compromised hosts (representing only 17.4% of our sample). The B-hosts bone union rate was 50.0%, while it reached 78.9% in A-hosts, but the difference was not statistically significant (p = .5392). Infection recurrence was higher in B-hosts than in A-hosts (p = .0086) and in Pseudomonas aeruginosa sustained infections (p = .0208), but in the latter case, the treatment strategy did not influence the outcome (p = .4000).
Conclusions
Bone union and infection healing rates are comparable between one and two-stage approaches. Pseudomonas aeruginosa infections have a higher risk of infection relapse, with similar effectiveness of one- and two-stage strategies. B-hosts have a higher infection recurrence rate without comparable data between the two approaches. Further studies with a larger sample size are required to confirm our results and define B-hosts' best strategy.
Level of Evidence
Level III of evidence, retrospective cohort study investigating the results of treatments.
期刊介绍:
Microsurgery is an international and interdisciplinary publication of original contributions concerning surgery under microscopic magnification. Microsurgery publishes clinical studies, research papers, invited articles, relevant reviews, and other scholarly works from all related fields including orthopaedic surgery, otolaryngology, pediatric surgery, plastic surgery, urology, and vascular surgery.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


