{"title":"曾接受过放射治疗的稳定脑转移灶与阿特珠单抗治疗非小细胞肺癌疗效的关系:对三项随机试验中单个患者数据的汇总分析。","authors":"Tiantian Guo, Yue Zhou, Fei Liang, Zezhou Wang, Vincent Bourbonne, Lukas Käsmann, Nora Sundahl, Abraham Jing-Ching Wu, Jianjiao Ni, Zhengfei Zhu","doi":"10.1002/cac2.12512","DOIUrl":null,"url":null,"abstract":"<p>Brain metastasis (BM) has long been recognized as a prognostic factor associated with poor prognosis for non-small cell lung cancer (NSCLC) in the era of conventional chemotherapy and targeted therapy [<span>1</span>]. In the era of immunotherapy, controversial findings have been reported regarding the prognostic significance of BM in patients with NSCLC treated with programmed death-1/programmed death-ligand 1 (PD-1/PD-L1) inhibitors. Several studies have shown that the presence of BM did not impact overall survival (OS) or progression-free survival (PFS) [<span>2, 3</span>], whereas other studies have identified BM as a negative prognostic factor [<span>4, 5</span>]. These previous works were mostly based on small sample sizes, and the prognostic significance of BM in patients treated with PD-1/PD-L1 inhibitors warrants further investigation.</p><p>In the present study, we used Vivli, a global, neutral data-sharing platform that enables access to anonymized individual patient data from trials, to evaluate the association between previously irradiated stable BM (iBM) and treatment outcomes of atezolizumab-containing regimens using pooled data from prospective phase III trials. Three clinical trials, IMpower130 (NCT02367781) [<span>6</span>], IMpower131 (NCT02367794) [<span>7</span>], and IMpower150 (NCT02366143) [<span>8</span>], were identified. Supplementary Table S1 provides an overview of the included three clinical trials. The study design and methods are described in the Supplementary Material.</p><p>Supplementary Figure S1 shows the patient disposition for the per-protocol population. In the per-protocol population (<i>n</i> = 2,700), only 10 (3.3%) of 316 patients with baseline BM did not undergo previous irradiation, who were excluded due to difficulties in statistical analyses. Among the 2,690 patients finally included, 210 (11.8%) of 1,778 patients in the atezolizumab-containing arm and 96 (10.5%) of 912 patients in the chemotherapy alone arm had iBM. Baseline demographics and clinical characteristics for patients without baseline BM and patients with iBM are shown in Supplementary Table S2. In patients without BM, OS and PFS were improved with atezolizumab-containing regimens compared with chemotherapy alone (Supplementary Figure S2). In patients with iBM, adding atezolizumab significantly improved OS and PFS compared with chemotherapy alone (Supplementary Figure S3).</p><p>We utilized propensity score matching (PSM) to control for the heterogeneity between patients with iBM and those without BM (Supplementary Table S3). A total of 11 patients in the atezolizumab-containing arm and 10 in the chemotherapy alone arm were excluded due to missing relevant baseline characteristic data. We compared the OS of patients with iBM and those without baseline BM before and after PSM (Figure 1). In the atezolizumab-containing arm, OS was longer in patients with iBM than in those without BM in the original cohort (unadjusted hazard ratio [HR] = 0.75, 95% confidence interval [CI] = 0.60-0.93, <i>P</i> = 0.011; adjusted HR = 0.75, 95% CI = 0.60–0.95, <i>P</i> = 0.015; Supplementary Table S4) and the propensity score-matched cohort (unadjusted HR = 0.35, 95% CI = 0.27-0.45, <i>P</i> < 0.001; adjusted HR = 0.26, 95% CI = 0.20–0.33, <i>P</i> < 0.001; Supplementary Table S5); in the chemotherapy alone arm, OS was similar between patients with iBM and those without BM in the original cohort and the propensity score-matched cohort. There was a significant interaction between treatment arms and BM status before and after PSM (<i>P</i><sub>interaction</sub> = 0.013, <i>P</i><sub>interaction</sub> < 0.001, respectively). We also applied stabilized inverse probability weighting and obtained similar results (Supplementary Table S6 and Supplementary Figure S4). We also compared the PFS of patients with iBM and those without baseline BM, and the results are shown in Supplementary Figures S5-S6 and Supplementary Tables S7-S10.</p><p>Furthermore, we compared the OS and PFS between patients without BM and patients with iBM who had radiotherapy technique information available and found that radiosurgery-treated stable BM or whole-brain radiotherapy-treated stable BM was associated with improved survival in the atezolizumab-containing arm after PSM, but not in those in the chemotherapy alone arm (Supplementary Figures S7-S10).</p><p>Atezolizumab-related neurological adverse events (AEs) of any grade occurred in 225 patients (14.3%) without baseline BM and 31 patients (14.8%) with iBM; atezolizumab-related grade 3/4 neurological AEs were reported in 19 patients (1.2%) without BM and 4 patients (1.9%) with iBM (Supplementary Table S11). The rates of atezolizumab-related serious neurological AEs were similar between patients without BM and patients with iBM (0.7% vs. 0.4%). The most common atezolizumab-related neurological AE was headache in patients without baseline BM and neuropathy peripheral in patients with iBM (Supplementary Table S12).</p><p>A unique feature of the present study compared to previous investigations is that all of the included patients with BM had previously received irradiation and had stable BM, whereas previous works included a heterogeneous group of BMs, including active BM, non-irradiated stable BM, and irradiated stable BM. Therefore, our findings hint at the possibility of the interaction of cranial radiotherapy with the immune system to augment anti-tumor immunity. Atezolizumab-containing chemoimmunotherapy combination has shown promising efficacy in NSCLC patients without BM. The better survival outcomes observed in patients with iBM who received atezolizumab-containing chemoimmunotherapy combination compared to those without BM may be due to the potential synergistic anti-tumor effects of cranial radiotherapy and atezolizumab. Cranial radiotherapy may have immunogenic effects on the tumor microenvironment of the brain, causing immunogenic cell death and the release of tumor antigens, which in turn activates immune cells. This immunogenic effect within the brain has the potential to enhance the systemic immune response to atezolizumab, leading to a more effective overall immune response. Further studies investigating if and how cranial radiotherapy could be a potential game-changer to prime a more effective systemic anti-tumor response to anti-PD-1/PD-L1 therapy for patients with BM are warranted.</p><p>There were some limitations of the present study. First, the small sample size of patients with non-irradiated BM did not allow for statistical comparisons of OS and PFS between patients with non-irradiated BM and those with iBM. It is worth mentioning that the presence of BM has been reported to have a negative prognostic impact or no significant effect on PFS or OS in patients with advanced NSCLC treated with PD-1/PD-L1 inhibitors [<span>2</span>-<span>5, 9, 10</span>]. In this regard, the significant survival benefit of patients with iBM compared to those without BM in the atezolizumab-containing arm is especially notable.</p><p>Second, since cranial radiotherapy was performed prior to enrollment, information on radiotherapy techniques was not available for 9.0% and 14.6% of the patients in the atezolizumab-containing arm and chemotherapy alone arm, respectively.</p><p>Third, this analysis was based on patients with treated stable BM. The prognostic significance of active BM in the era of immunotherapy is largely unknown since patients with active BM are excluded in almost all of the clinical trials. Additionally, the three trials included in the present study utilized different therapeutic agents in addition to atezolizumab, which could potentially introduce a confounding factor.</p><p>Overall, our results suggest that previously irradiated stable BM was associated with improved outcomes in patients who received atezolizumab-containing regimens. These data lend credence to the notion that even though anti-PD-1/PD-L1 therapy has activity against BM, patients may benefit from having cranial radiotherapy prior to anti-PD-1/PD-L1 therapy. Our findings also highlight the need to explore whether cranial radiotherapy can improve systemic responses to immunotherapy in patients with BM from NSCLC.</p><p>Study conception and design: TG, JN, ZZ. Data acquisition: TG, JN, ZZ, YZ. Data analyses: TG, JN, FL, ZW. Data interpretation: all authors; contribution to and approval of manuscript: all authors.</p><p>None declared.</p><p>Chinese Society of Clinical Oncology (Y-BM2019-082, Y-MSD2020-0147), Science and Technology Commission of Shanghai Municipality (20Y11913500).</p><p>Not required.</p><p>This study was deemed negligible risk research and exempt from review by the Ethical Committees of Fudan University Shanghai Cancer Center.</p>","PeriodicalId":9495,"journal":{"name":"Cancer Communications","volume":"44 2","pages":"278-281"},"PeriodicalIF":20.1000,"publicationDate":"2023-12-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cac2.12512","citationCount":"0","resultStr":"{\"title\":\"Association of previously irradiated stable brain metastases with outcomes of atezolizumab-treated non-small cell lung cancer: A pooled analysis of individual patient data from three randomized trials\",\"authors\":\"Tiantian Guo, Yue Zhou, Fei Liang, Zezhou Wang, Vincent Bourbonne, Lukas Käsmann, Nora Sundahl, Abraham Jing-Ching Wu, Jianjiao Ni, Zhengfei Zhu\",\"doi\":\"10.1002/cac2.12512\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Brain metastasis (BM) has long been recognized as a prognostic factor associated with poor prognosis for non-small cell lung cancer (NSCLC) in the era of conventional chemotherapy and targeted therapy [<span>1</span>]. In the era of immunotherapy, controversial findings have been reported regarding the prognostic significance of BM in patients with NSCLC treated with programmed death-1/programmed death-ligand 1 (PD-1/PD-L1) inhibitors. Several studies have shown that the presence of BM did not impact overall survival (OS) or progression-free survival (PFS) [<span>2, 3</span>], whereas other studies have identified BM as a negative prognostic factor [<span>4, 5</span>]. These previous works were mostly based on small sample sizes, and the prognostic significance of BM in patients treated with PD-1/PD-L1 inhibitors warrants further investigation.</p><p>In the present study, we used Vivli, a global, neutral data-sharing platform that enables access to anonymized individual patient data from trials, to evaluate the association between previously irradiated stable BM (iBM) and treatment outcomes of atezolizumab-containing regimens using pooled data from prospective phase III trials. Three clinical trials, IMpower130 (NCT02367781) [<span>6</span>], IMpower131 (NCT02367794) [<span>7</span>], and IMpower150 (NCT02366143) [<span>8</span>], were identified. Supplementary Table S1 provides an overview of the included three clinical trials. The study design and methods are described in the Supplementary Material.</p><p>Supplementary Figure S1 shows the patient disposition for the per-protocol population. In the per-protocol population (<i>n</i> = 2,700), only 10 (3.3%) of 316 patients with baseline BM did not undergo previous irradiation, who were excluded due to difficulties in statistical analyses. Among the 2,690 patients finally included, 210 (11.8%) of 1,778 patients in the atezolizumab-containing arm and 96 (10.5%) of 912 patients in the chemotherapy alone arm had iBM. Baseline demographics and clinical characteristics for patients without baseline BM and patients with iBM are shown in Supplementary Table S2. In patients without BM, OS and PFS were improved with atezolizumab-containing regimens compared with chemotherapy alone (Supplementary Figure S2). In patients with iBM, adding atezolizumab significantly improved OS and PFS compared with chemotherapy alone (Supplementary Figure S3).</p><p>We utilized propensity score matching (PSM) to control for the heterogeneity between patients with iBM and those without BM (Supplementary Table S3). A total of 11 patients in the atezolizumab-containing arm and 10 in the chemotherapy alone arm were excluded due to missing relevant baseline characteristic data. We compared the OS of patients with iBM and those without baseline BM before and after PSM (Figure 1). In the atezolizumab-containing arm, OS was longer in patients with iBM than in those without BM in the original cohort (unadjusted hazard ratio [HR] = 0.75, 95% confidence interval [CI] = 0.60-0.93, <i>P</i> = 0.011; adjusted HR = 0.75, 95% CI = 0.60–0.95, <i>P</i> = 0.015; Supplementary Table S4) and the propensity score-matched cohort (unadjusted HR = 0.35, 95% CI = 0.27-0.45, <i>P</i> < 0.001; adjusted HR = 0.26, 95% CI = 0.20–0.33, <i>P</i> < 0.001; Supplementary Table S5); in the chemotherapy alone arm, OS was similar between patients with iBM and those without BM in the original cohort and the propensity score-matched cohort. There was a significant interaction between treatment arms and BM status before and after PSM (<i>P</i><sub>interaction</sub> = 0.013, <i>P</i><sub>interaction</sub> < 0.001, respectively). We also applied stabilized inverse probability weighting and obtained similar results (Supplementary Table S6 and Supplementary Figure S4). We also compared the PFS of patients with iBM and those without baseline BM, and the results are shown in Supplementary Figures S5-S6 and Supplementary Tables S7-S10.</p><p>Furthermore, we compared the OS and PFS between patients without BM and patients with iBM who had radiotherapy technique information available and found that radiosurgery-treated stable BM or whole-brain radiotherapy-treated stable BM was associated with improved survival in the atezolizumab-containing arm after PSM, but not in those in the chemotherapy alone arm (Supplementary Figures S7-S10).</p><p>Atezolizumab-related neurological adverse events (AEs) of any grade occurred in 225 patients (14.3%) without baseline BM and 31 patients (14.8%) with iBM; atezolizumab-related grade 3/4 neurological AEs were reported in 19 patients (1.2%) without BM and 4 patients (1.9%) with iBM (Supplementary Table S11). The rates of atezolizumab-related serious neurological AEs were similar between patients without BM and patients with iBM (0.7% vs. 0.4%). The most common atezolizumab-related neurological AE was headache in patients without baseline BM and neuropathy peripheral in patients with iBM (Supplementary Table S12).</p><p>A unique feature of the present study compared to previous investigations is that all of the included patients with BM had previously received irradiation and had stable BM, whereas previous works included a heterogeneous group of BMs, including active BM, non-irradiated stable BM, and irradiated stable BM. Therefore, our findings hint at the possibility of the interaction of cranial radiotherapy with the immune system to augment anti-tumor immunity. Atezolizumab-containing chemoimmunotherapy combination has shown promising efficacy in NSCLC patients without BM. The better survival outcomes observed in patients with iBM who received atezolizumab-containing chemoimmunotherapy combination compared to those without BM may be due to the potential synergistic anti-tumor effects of cranial radiotherapy and atezolizumab. Cranial radiotherapy may have immunogenic effects on the tumor microenvironment of the brain, causing immunogenic cell death and the release of tumor antigens, which in turn activates immune cells. This immunogenic effect within the brain has the potential to enhance the systemic immune response to atezolizumab, leading to a more effective overall immune response. Further studies investigating if and how cranial radiotherapy could be a potential game-changer to prime a more effective systemic anti-tumor response to anti-PD-1/PD-L1 therapy for patients with BM are warranted.</p><p>There were some limitations of the present study. First, the small sample size of patients with non-irradiated BM did not allow for statistical comparisons of OS and PFS between patients with non-irradiated BM and those with iBM. It is worth mentioning that the presence of BM has been reported to have a negative prognostic impact or no significant effect on PFS or OS in patients with advanced NSCLC treated with PD-1/PD-L1 inhibitors [<span>2</span>-<span>5, 9, 10</span>]. In this regard, the significant survival benefit of patients with iBM compared to those without BM in the atezolizumab-containing arm is especially notable.</p><p>Second, since cranial radiotherapy was performed prior to enrollment, information on radiotherapy techniques was not available for 9.0% and 14.6% of the patients in the atezolizumab-containing arm and chemotherapy alone arm, respectively.</p><p>Third, this analysis was based on patients with treated stable BM. The prognostic significance of active BM in the era of immunotherapy is largely unknown since patients with active BM are excluded in almost all of the clinical trials. Additionally, the three trials included in the present study utilized different therapeutic agents in addition to atezolizumab, which could potentially introduce a confounding factor.</p><p>Overall, our results suggest that previously irradiated stable BM was associated with improved outcomes in patients who received atezolizumab-containing regimens. These data lend credence to the notion that even though anti-PD-1/PD-L1 therapy has activity against BM, patients may benefit from having cranial radiotherapy prior to anti-PD-1/PD-L1 therapy. Our findings also highlight the need to explore whether cranial radiotherapy can improve systemic responses to immunotherapy in patients with BM from NSCLC.</p><p>Study conception and design: TG, JN, ZZ. Data acquisition: TG, JN, ZZ, YZ. Data analyses: TG, JN, FL, ZW. Data interpretation: all authors; contribution to and approval of manuscript: all authors.</p><p>None declared.</p><p>Chinese Society of Clinical Oncology (Y-BM2019-082, Y-MSD2020-0147), Science and Technology Commission of Shanghai Municipality (20Y11913500).</p><p>Not required.</p><p>This study was deemed negligible risk research and exempt from review by the Ethical Committees of Fudan University Shanghai Cancer Center.</p>\",\"PeriodicalId\":9495,\"journal\":{\"name\":\"Cancer Communications\",\"volume\":\"44 2\",\"pages\":\"278-281\"},\"PeriodicalIF\":20.1000,\"publicationDate\":\"2023-12-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cac2.12512\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cancer Communications\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/cac2.12512\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancer Communications","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cac2.12512","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
在传统化疗和靶向治疗时代,脑转移(BM)一直被认为是与非小细胞肺癌(NSCLC)不良预后相关的预后因素[1]。在免疫疗法时代,关于程序性死亡-1/程序性死亡配体 1(PD-1/PD-L1)抑制剂治疗的 NSCLC 患者 BM 的预后意义,已有争议性的研究结果。一些研究表明,BM 的存在并不影响总生存期(OS)或无进展生存期(PFS)[2, 3],而另一些研究则认为 BM 是一个负面的预后因素[4, 5]。在本研究中,我们使用 Vivli(一个全球性、中立的数据共享平台,可访问试验中匿名的患者个体数据),利用前瞻性 III 期试验的汇总数据评估了既往照射过的稳定 BM(iBM)与含阿特珠单抗方案治疗结果之间的关联。共确定了三项临床试验:IMpower130(NCT02367781)[6]、IMpower131(NCT02367794)[7]和IMpower150(NCT02366143)[8]。补充表 S1 提供了所纳入的三项临床试验的概况。研究设计和方法见补充材料。补充图 S1 显示了按协议人群的患者处置情况。在按协议人群(n = 2,700)中,基线BM的316名患者中仅有10人(3.3%)既往未接受过照射,由于统计分析困难而被排除在外。在最终纳入的 2,690 名患者中,含阿替珠单抗治疗组的 1,778 名患者中有 210 人(11.8%)患有 iBM,而单纯化疗组的 912 名患者中有 96 人(10.5%)患有 iBM。无基线BM患者和有iBM患者的基线人口统计学特征和临床特征见补充表S2。与单纯化疗相比,在无基础骨髓瘤的患者中,使用含有阿特珠单抗的方案可改善OS和PFS(补充图S2)。在iBM患者中,与单纯化疗相比,添加atezolizumab能显著改善OS和PFS(补充图S3)。我们利用倾向评分匹配(PSM)来控制iBM患者与无BM患者之间的异质性(补充表S3)。由于缺失相关基线特征数据,共排除了含阿替珠单抗治疗组的11例患者和单纯化疗组的10例患者。我们比较了iBM患者和无基线BM患者在PSM前后的OS(图1)。在含有阿特珠单抗的治疗组中,原始队列中的iBM患者的OS长于无BM患者(未经调整的危险比[HR] = 0.75,95%置信区间[CI] = 0.60-0.93,P = 0.011;调整后的HR = 0.75,95% CI = 0.60-0.95,P = 0.015;补充表S4),倾向评分匹配队列中的iBM患者的OS也长于无BM患者(未经调整的HR = 0.35, 95% CI = 0.27-0.45, P < 0.001; 调整后 HR = 0.26, 95% CI = 0.20-0.33, P < 0.001; 补充表 S5);在单纯化疗组中,原始队列和倾向评分匹配队列中的 iBM 患者与无 BM 患者的 OS 相似。在 PSM 前后,治疗组与 BM 状态之间存在明显的交互作用(Pinteraction = 0.013,Pinteraction < 0.001)。我们还应用了稳定的反概率加权法,得到了相似的结果(补充表 S6 和补充图 S4)。我们还比较了有 iBM 和无基线 BM 患者的 PFS,结果见补充图 S5-S6 和补充表 S7-S10。此外,我们还比较了无BM患者和有放疗技术信息的iBM患者的OS和PFS,发现放射外科治疗的稳定BM或全脑放疗治疗的稳定BM与PSM后含阿特珠单抗组生存率的改善有关,但与单纯化疗组无关(补充图S7-S10)。225例(14.3%)无基线BM的患者和31例(14.8%)iBM患者发生了任何级别的阿特珠单抗相关神经系统不良事件(AEs);19例(1.2%)无基线BM的患者和4例(1.9%)iBM患者发生了阿特珠单抗相关的3/4级神经系统不良事件(补充表S11)。无BM患者和iBM患者发生atezolizumab相关严重神经系统AEs的比例相似(0.7% vs. 0.4%)。最常见的atezolizumab相关神经系统AE是无基线BM患者的头痛和iBM患者的周围神经病变(补充表S12)。
Association of previously irradiated stable brain metastases with outcomes of atezolizumab-treated non-small cell lung cancer: A pooled analysis of individual patient data from three randomized trials
Brain metastasis (BM) has long been recognized as a prognostic factor associated with poor prognosis for non-small cell lung cancer (NSCLC) in the era of conventional chemotherapy and targeted therapy [1]. In the era of immunotherapy, controversial findings have been reported regarding the prognostic significance of BM in patients with NSCLC treated with programmed death-1/programmed death-ligand 1 (PD-1/PD-L1) inhibitors. Several studies have shown that the presence of BM did not impact overall survival (OS) or progression-free survival (PFS) [2, 3], whereas other studies have identified BM as a negative prognostic factor [4, 5]. These previous works were mostly based on small sample sizes, and the prognostic significance of BM in patients treated with PD-1/PD-L1 inhibitors warrants further investigation.
In the present study, we used Vivli, a global, neutral data-sharing platform that enables access to anonymized individual patient data from trials, to evaluate the association between previously irradiated stable BM (iBM) and treatment outcomes of atezolizumab-containing regimens using pooled data from prospective phase III trials. Three clinical trials, IMpower130 (NCT02367781) [6], IMpower131 (NCT02367794) [7], and IMpower150 (NCT02366143) [8], were identified. Supplementary Table S1 provides an overview of the included three clinical trials. The study design and methods are described in the Supplementary Material.
Supplementary Figure S1 shows the patient disposition for the per-protocol population. In the per-protocol population (n = 2,700), only 10 (3.3%) of 316 patients with baseline BM did not undergo previous irradiation, who were excluded due to difficulties in statistical analyses. Among the 2,690 patients finally included, 210 (11.8%) of 1,778 patients in the atezolizumab-containing arm and 96 (10.5%) of 912 patients in the chemotherapy alone arm had iBM. Baseline demographics and clinical characteristics for patients without baseline BM and patients with iBM are shown in Supplementary Table S2. In patients without BM, OS and PFS were improved with atezolizumab-containing regimens compared with chemotherapy alone (Supplementary Figure S2). In patients with iBM, adding atezolizumab significantly improved OS and PFS compared with chemotherapy alone (Supplementary Figure S3).
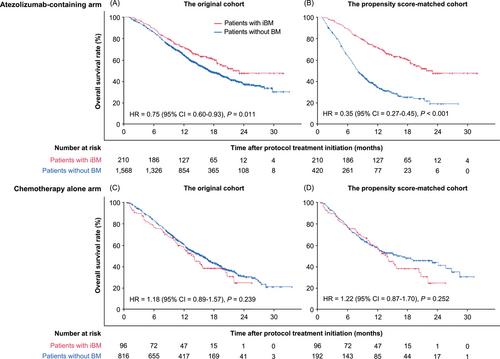
We utilized propensity score matching (PSM) to control for the heterogeneity between patients with iBM and those without BM (Supplementary Table S3). A total of 11 patients in the atezolizumab-containing arm and 10 in the chemotherapy alone arm were excluded due to missing relevant baseline characteristic data. We compared the OS of patients with iBM and those without baseline BM before and after PSM (Figure 1). In the atezolizumab-containing arm, OS was longer in patients with iBM than in those without BM in the original cohort (unadjusted hazard ratio [HR] = 0.75, 95% confidence interval [CI] = 0.60-0.93, P = 0.011; adjusted HR = 0.75, 95% CI = 0.60–0.95, P = 0.015; Supplementary Table S4) and the propensity score-matched cohort (unadjusted HR = 0.35, 95% CI = 0.27-0.45, P < 0.001; adjusted HR = 0.26, 95% CI = 0.20–0.33, P < 0.001; Supplementary Table S5); in the chemotherapy alone arm, OS was similar between patients with iBM and those without BM in the original cohort and the propensity score-matched cohort. There was a significant interaction between treatment arms and BM status before and after PSM (Pinteraction = 0.013, Pinteraction < 0.001, respectively). We also applied stabilized inverse probability weighting and obtained similar results (Supplementary Table S6 and Supplementary Figure S4). We also compared the PFS of patients with iBM and those without baseline BM, and the results are shown in Supplementary Figures S5-S6 and Supplementary Tables S7-S10.
Furthermore, we compared the OS and PFS between patients without BM and patients with iBM who had radiotherapy technique information available and found that radiosurgery-treated stable BM or whole-brain radiotherapy-treated stable BM was associated with improved survival in the atezolizumab-containing arm after PSM, but not in those in the chemotherapy alone arm (Supplementary Figures S7-S10).
Atezolizumab-related neurological adverse events (AEs) of any grade occurred in 225 patients (14.3%) without baseline BM and 31 patients (14.8%) with iBM; atezolizumab-related grade 3/4 neurological AEs were reported in 19 patients (1.2%) without BM and 4 patients (1.9%) with iBM (Supplementary Table S11). The rates of atezolizumab-related serious neurological AEs were similar between patients without BM and patients with iBM (0.7% vs. 0.4%). The most common atezolizumab-related neurological AE was headache in patients without baseline BM and neuropathy peripheral in patients with iBM (Supplementary Table S12).
A unique feature of the present study compared to previous investigations is that all of the included patients with BM had previously received irradiation and had stable BM, whereas previous works included a heterogeneous group of BMs, including active BM, non-irradiated stable BM, and irradiated stable BM. Therefore, our findings hint at the possibility of the interaction of cranial radiotherapy with the immune system to augment anti-tumor immunity. Atezolizumab-containing chemoimmunotherapy combination has shown promising efficacy in NSCLC patients without BM. The better survival outcomes observed in patients with iBM who received atezolizumab-containing chemoimmunotherapy combination compared to those without BM may be due to the potential synergistic anti-tumor effects of cranial radiotherapy and atezolizumab. Cranial radiotherapy may have immunogenic effects on the tumor microenvironment of the brain, causing immunogenic cell death and the release of tumor antigens, which in turn activates immune cells. This immunogenic effect within the brain has the potential to enhance the systemic immune response to atezolizumab, leading to a more effective overall immune response. Further studies investigating if and how cranial radiotherapy could be a potential game-changer to prime a more effective systemic anti-tumor response to anti-PD-1/PD-L1 therapy for patients with BM are warranted.
There were some limitations of the present study. First, the small sample size of patients with non-irradiated BM did not allow for statistical comparisons of OS and PFS between patients with non-irradiated BM and those with iBM. It is worth mentioning that the presence of BM has been reported to have a negative prognostic impact or no significant effect on PFS or OS in patients with advanced NSCLC treated with PD-1/PD-L1 inhibitors [2-5, 9, 10]. In this regard, the significant survival benefit of patients with iBM compared to those without BM in the atezolizumab-containing arm is especially notable.
Second, since cranial radiotherapy was performed prior to enrollment, information on radiotherapy techniques was not available for 9.0% and 14.6% of the patients in the atezolizumab-containing arm and chemotherapy alone arm, respectively.
Third, this analysis was based on patients with treated stable BM. The prognostic significance of active BM in the era of immunotherapy is largely unknown since patients with active BM are excluded in almost all of the clinical trials. Additionally, the three trials included in the present study utilized different therapeutic agents in addition to atezolizumab, which could potentially introduce a confounding factor.
Overall, our results suggest that previously irradiated stable BM was associated with improved outcomes in patients who received atezolizumab-containing regimens. These data lend credence to the notion that even though anti-PD-1/PD-L1 therapy has activity against BM, patients may benefit from having cranial radiotherapy prior to anti-PD-1/PD-L1 therapy. Our findings also highlight the need to explore whether cranial radiotherapy can improve systemic responses to immunotherapy in patients with BM from NSCLC.
Study conception and design: TG, JN, ZZ. Data acquisition: TG, JN, ZZ, YZ. Data analyses: TG, JN, FL, ZW. Data interpretation: all authors; contribution to and approval of manuscript: all authors.
None declared.
Chinese Society of Clinical Oncology (Y-BM2019-082, Y-MSD2020-0147), Science and Technology Commission of Shanghai Municipality (20Y11913500).
Not required.
This study was deemed negligible risk research and exempt from review by the Ethical Committees of Fudan University Shanghai Cancer Center.
期刊介绍:
Cancer Communications is an open access, peer-reviewed online journal that encompasses basic, clinical, and translational cancer research. The journal welcomes submissions concerning clinical trials, epidemiology, molecular and cellular biology, and genetics.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


