{"title":"接受同种异体造血干细胞移植治疗移植物抗宿主病的儿童患者给予甲氨蝶呤后他克莫司浓度升高。","authors":"Chiaki Inoue, Takehito Yamamoto, Hiroshi Miyata, Hiroshi Suzuki, Tappei Takada","doi":"10.1186/s40780-023-00306-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Methotrexate (MTX) is used to treat graft-versus-host disease (GVHD) following allogeneic hematopoietic stem cell transplantation (allo-HSCT). Recently, a case was encountered in which the blood concentration of tacrolimus (TCR) at steady state increased after intravenous MTX administration for GVHD treatment (therapeutic IV-MTX administration). Therefore, this study aimed to investigate the effect of therapeutic IV-MTX administration on the pharmacokinetics of TCR.</p><p><strong>Methods: </strong>This single-center, retrospective, observational study included patients who underwent allo-HSCT and received therapeutic IV-MTX administration during immunosuppressive therapy with continuous intravenous infusion (CIV) of TCR from April 2004 to December 2021. Here, each therapeutic IV-MTX administration was defined as a case and independently subjected to subsequent analyses. The blood concentration of TCR at steady state (C<sub>ss</sub>), ratio of C<sub>ss</sub> to daily TCR dose (C/D), and clinical laboratory data were compared before and after therapeutic IV-MTX administration. In addition, dose changes in the TCR after therapeutic IV-MTX administration were evaluated.</p><p><strong>Results: </strong>Ten patients (23 cases) were included in this study. The C/D value significantly increased after therapeutic IV-MTX administration (median: 697 vs. 771 (ng/mL)/(mg/kg), 1.16-fold increase, P < 0.05), indicating a reduction in the apparent clearance of TCR. Along with the increase in C/D, significant increases were observed in aspartate transaminase level (median: 51.0 vs. 92.9 U/L, P < 0.01) and alanine aminotransferase level (median: 74.5 vs. 99.4 U/L, P < 0.01) indicating that liver injury after therapeutic IV-MTX administration contributes to the observed C/D increase. In addition, the daily dose of TCR was reduced in 11 cases (47.8%) after therapeutic IV-MTX administration, and the relative frequency of dose reduction tended to be higher than that of dose increase (median: 37.5% vs. 0.0%, P = 0.0519, permuted Brunner-Munzel test). The magnitude of dose reduction was 18.8% (7.4-50.0%) in the 11 cases with dose reduction.</p><p><strong>Conclusions: </strong>Therapeutic IV-MTX administration cause a significant increase in C/D, which requires TCR dose reduction. Careful therapeutic drug monitoring of TCR is needed after therapeutic IV-MTX administration in patients receiving immunosuppressive therapy with TCR after allo-HSCT.</p>","PeriodicalId":16730,"journal":{"name":"Journal of Pharmaceutical Health Care and Sciences","volume":"9 1","pages":"38"},"PeriodicalIF":1.2000,"publicationDate":"2023-12-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10696830/pdf/","citationCount":"0","resultStr":"{\"title\":\"Elevation of tacrolimus concentration after administration of methotrexate for treatment of graft-versus-host disease in pediatric patients received allogeneic hematopoietic stem cell transplantation.\",\"authors\":\"Chiaki Inoue, Takehito Yamamoto, Hiroshi Miyata, Hiroshi Suzuki, Tappei Takada\",\"doi\":\"10.1186/s40780-023-00306-w\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Methotrexate (MTX) is used to treat graft-versus-host disease (GVHD) following allogeneic hematopoietic stem cell transplantation (allo-HSCT). Recently, a case was encountered in which the blood concentration of tacrolimus (TCR) at steady state increased after intravenous MTX administration for GVHD treatment (therapeutic IV-MTX administration). Therefore, this study aimed to investigate the effect of therapeutic IV-MTX administration on the pharmacokinetics of TCR.</p><p><strong>Methods: </strong>This single-center, retrospective, observational study included patients who underwent allo-HSCT and received therapeutic IV-MTX administration during immunosuppressive therapy with continuous intravenous infusion (CIV) of TCR from April 2004 to December 2021. Here, each therapeutic IV-MTX administration was defined as a case and independently subjected to subsequent analyses. The blood concentration of TCR at steady state (C<sub>ss</sub>), ratio of C<sub>ss</sub> to daily TCR dose (C/D), and clinical laboratory data were compared before and after therapeutic IV-MTX administration. In addition, dose changes in the TCR after therapeutic IV-MTX administration were evaluated.</p><p><strong>Results: </strong>Ten patients (23 cases) were included in this study. The C/D value significantly increased after therapeutic IV-MTX administration (median: 697 vs. 771 (ng/mL)/(mg/kg), 1.16-fold increase, P < 0.05), indicating a reduction in the apparent clearance of TCR. Along with the increase in C/D, significant increases were observed in aspartate transaminase level (median: 51.0 vs. 92.9 U/L, P < 0.01) and alanine aminotransferase level (median: 74.5 vs. 99.4 U/L, P < 0.01) indicating that liver injury after therapeutic IV-MTX administration contributes to the observed C/D increase. In addition, the daily dose of TCR was reduced in 11 cases (47.8%) after therapeutic IV-MTX administration, and the relative frequency of dose reduction tended to be higher than that of dose increase (median: 37.5% vs. 0.0%, P = 0.0519, permuted Brunner-Munzel test). The magnitude of dose reduction was 18.8% (7.4-50.0%) in the 11 cases with dose reduction.</p><p><strong>Conclusions: </strong>Therapeutic IV-MTX administration cause a significant increase in C/D, which requires TCR dose reduction. Careful therapeutic drug monitoring of TCR is needed after therapeutic IV-MTX administration in patients receiving immunosuppressive therapy with TCR after allo-HSCT.</p>\",\"PeriodicalId\":16730,\"journal\":{\"name\":\"Journal of Pharmaceutical Health Care and Sciences\",\"volume\":\"9 1\",\"pages\":\"38\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2023-12-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10696830/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Pharmaceutical Health Care and Sciences\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s40780-023-00306-w\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Pharmaceutical Health Care and Sciences","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40780-023-00306-w","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
摘要
背景:甲氨蝶呤(MTX)用于治疗同种异体造血干细胞移植后的移植物抗宿主病(GVHD)。最近报道了一例静脉给药MTX治疗GVHD(治疗性IV-MTX给药)后他克莫司(TCR)稳态血药浓度升高的病例。因此,本研究旨在探讨IV-MTX治疗性给药对TCR药代动力学的影响。方法:这项单中心、回顾性、观察性研究纳入了2004年4月至2021年12月接受同种异体造血干细胞移植并在持续静脉输注TCR (CIV)免疫抑制治疗期间接受IV-MTX治疗的患者。在这里,每次IV-MTX治疗被定义为一个病例,并独立地进行后续分析。比较IV-MTX治疗前后TCR稳态血药浓度(Css)、Css与TCR日剂量之比(C/D)及临床实验室数据。此外,评估IV-MTX治疗后TCR的剂量变化。结果:10例患者(23例)纳入本研究。IV-MTX治疗性给药后C/D值显著升高(中位数:697 vs. 771 (ng/mL)/(mg/kg),增加1.16倍,P结论:IV-MTX治疗性给药导致C/D显著升高,需要减少TCR剂量。对于同种异体造血干细胞移植后接受TCR免疫抑制治疗的患者,在给予IV-MTX治疗性治疗后,需要仔细监测TCR。
Elevation of tacrolimus concentration after administration of methotrexate for treatment of graft-versus-host disease in pediatric patients received allogeneic hematopoietic stem cell transplantation.
Background: Methotrexate (MTX) is used to treat graft-versus-host disease (GVHD) following allogeneic hematopoietic stem cell transplantation (allo-HSCT). Recently, a case was encountered in which the blood concentration of tacrolimus (TCR) at steady state increased after intravenous MTX administration for GVHD treatment (therapeutic IV-MTX administration). Therefore, this study aimed to investigate the effect of therapeutic IV-MTX administration on the pharmacokinetics of TCR.
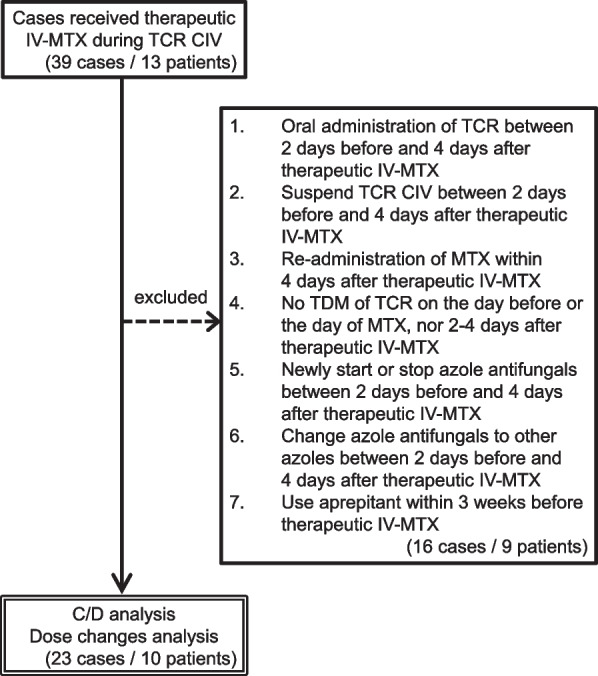
Methods: This single-center, retrospective, observational study included patients who underwent allo-HSCT and received therapeutic IV-MTX administration during immunosuppressive therapy with continuous intravenous infusion (CIV) of TCR from April 2004 to December 2021. Here, each therapeutic IV-MTX administration was defined as a case and independently subjected to subsequent analyses. The blood concentration of TCR at steady state (Css), ratio of Css to daily TCR dose (C/D), and clinical laboratory data were compared before and after therapeutic IV-MTX administration. In addition, dose changes in the TCR after therapeutic IV-MTX administration were evaluated.
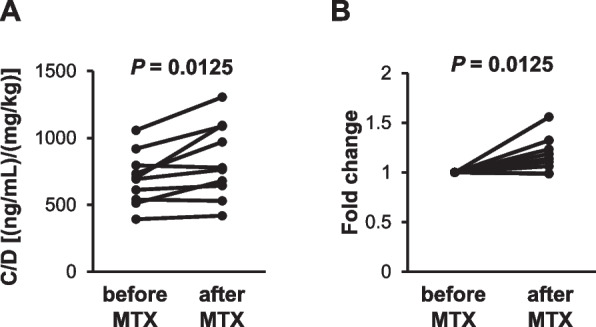
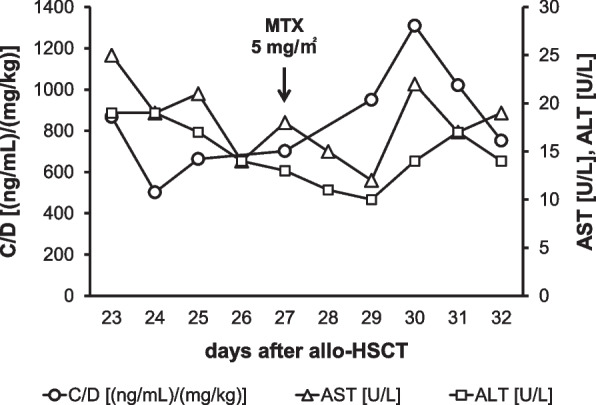
Results: Ten patients (23 cases) were included in this study. The C/D value significantly increased after therapeutic IV-MTX administration (median: 697 vs. 771 (ng/mL)/(mg/kg), 1.16-fold increase, P < 0.05), indicating a reduction in the apparent clearance of TCR. Along with the increase in C/D, significant increases were observed in aspartate transaminase level (median: 51.0 vs. 92.9 U/L, P < 0.01) and alanine aminotransferase level (median: 74.5 vs. 99.4 U/L, P < 0.01) indicating that liver injury after therapeutic IV-MTX administration contributes to the observed C/D increase. In addition, the daily dose of TCR was reduced in 11 cases (47.8%) after therapeutic IV-MTX administration, and the relative frequency of dose reduction tended to be higher than that of dose increase (median: 37.5% vs. 0.0%, P = 0.0519, permuted Brunner-Munzel test). The magnitude of dose reduction was 18.8% (7.4-50.0%) in the 11 cases with dose reduction.
Conclusions: Therapeutic IV-MTX administration cause a significant increase in C/D, which requires TCR dose reduction. Careful therapeutic drug monitoring of TCR is needed after therapeutic IV-MTX administration in patients receiving immunosuppressive therapy with TCR after allo-HSCT.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


