Janet Bouttell, Heather Fraser, John R. Goodlad, David Hopkins, Pam McKay, Karin A. Oien, Bruce Seligmann, Stephan von Delft, Neil Hawkins
{"title":"增加基因表达谱测试以帮助侵袭性大b细胞淋巴瘤的鉴别诊断和治疗:早期探索性经济评估。","authors":"Janet Bouttell, Heather Fraser, John R. Goodlad, David Hopkins, Pam McKay, Karin A. Oien, Bruce Seligmann, Stephan von Delft, Neil Hawkins","doi":"10.1007/s40258-023-00845-1","DOIUrl":null,"url":null,"abstract":"<div><h3>Background and Objective</h3><p>Adding gene expression profiles (GEPs) to the current diagnostic work-up of aggressive large B-cell lymphomas may lead to the reclassification of patients, treatment changes and improved outcomes. A GEP test is in development using TempO-Seq<sup>®</sup> technology to distinguish Burkitt lymphoma (BL) and primary mediastinal large B-cell lymphoma (PMBCL) from diffuse large B-cell lymphoma (DLBCL), and to classify patients with DLBLC and to predict the benefit of (e.g.) adding bortezomib to R-CHOP therapy (RB-CHOP). This study aims to estimate the potential impact of a GEP test on costs and health outcomes to inform pricing and evidence generation strategies.</p><h3>Methods</h3><p>Three decision models were developed comparing diagnostic strategies with and without GEP signatures over a lifetime horizon using a UK health and social care perspective. Inputs were taken from a recent clinical trial, literature and expert opinion. We estimated the maximum price of the test using a threshold of Great Britain Pound (GBP) 30,000 per quality-adjusted life-year (QALY). Sensitivity analyses were conducted.</p><h3>Results</h3><p>The estimated maximum threshold price for a combined test to be cost effective is GBP 15,352. At base-case values, the BL signature delivers QALY gains of 0.054 at an additional cost of GBP 275. This results in a net monetary benefit at a threshold of GBP 30,000 per QALY of GBP 1345. For PMBCL, the QALY gain was 0.0011 at a cost saving of GBP 406 and the net monetary benefit was GBP 437. The hazard ratio for the impact of treating BL less intensively must be at least 1.2 for a positive net monetary benefit. For identifying patients with the DLBCL subtype responsive to bortezomib, QALY gain was 0.2465 at a cost saving of GBP 6175, resulting in a net monetary benefit of GBP 13,570. In a probabilistic sensitivity analysis using 1000 simulations, a testing strategy was superior to a treat all with R-CHOP strategy in 81% of the simulations and with a cost saving in 92% assuming a cost price of zero.</p><h3>Conclusions</h3><p>Our estimates show that the combined test has a high probability of being cost effective. There is good quality evidence for the benefit of subtyping DLBCL but the evidence on the number of patients reclassified to or from BL and PMBCL and the impact of a more precise diagnosis and the cost of treatment is weak. The developers can use the price estimate to inform a return on investment calculations. Evidence will be required of how well the TempO-Seq<sup>®</sup> technology performs compared to the testing GEP technology used for subtyping in the recent clinical trial. For BL and PMBCL elements of the test, evidence would be required of the number of patients reclassified and improved costing information would be useful. The diagnostic and therapeutic environment in haematological malignancies is fast moving, which increases the risk for developers of diagnostic tests.</p></div>","PeriodicalId":8065,"journal":{"name":"Applied Health Economics and Health Policy","volume":"22 2","pages":"243 - 254"},"PeriodicalIF":3.1000,"publicationDate":"2023-11-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Adding a Gene Expression Profile Test to Aid Differential Diagnosis and Treatment in Aggressive Large B-Cell Lymphoma: An Early Exploratory Economic Evaluation\",\"authors\":\"Janet Bouttell, Heather Fraser, John R. Goodlad, David Hopkins, Pam McKay, Karin A. Oien, Bruce Seligmann, Stephan von Delft, Neil Hawkins\",\"doi\":\"10.1007/s40258-023-00845-1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background and Objective</h3><p>Adding gene expression profiles (GEPs) to the current diagnostic work-up of aggressive large B-cell lymphomas may lead to the reclassification of patients, treatment changes and improved outcomes. A GEP test is in development using TempO-Seq<sup>®</sup> technology to distinguish Burkitt lymphoma (BL) and primary mediastinal large B-cell lymphoma (PMBCL) from diffuse large B-cell lymphoma (DLBCL), and to classify patients with DLBLC and to predict the benefit of (e.g.) adding bortezomib to R-CHOP therapy (RB-CHOP). This study aims to estimate the potential impact of a GEP test on costs and health outcomes to inform pricing and evidence generation strategies.</p><h3>Methods</h3><p>Three decision models were developed comparing diagnostic strategies with and without GEP signatures over a lifetime horizon using a UK health and social care perspective. Inputs were taken from a recent clinical trial, literature and expert opinion. We estimated the maximum price of the test using a threshold of Great Britain Pound (GBP) 30,000 per quality-adjusted life-year (QALY). Sensitivity analyses were conducted.</p><h3>Results</h3><p>The estimated maximum threshold price for a combined test to be cost effective is GBP 15,352. At base-case values, the BL signature delivers QALY gains of 0.054 at an additional cost of GBP 275. This results in a net monetary benefit at a threshold of GBP 30,000 per QALY of GBP 1345. For PMBCL, the QALY gain was 0.0011 at a cost saving of GBP 406 and the net monetary benefit was GBP 437. The hazard ratio for the impact of treating BL less intensively must be at least 1.2 for a positive net monetary benefit. For identifying patients with the DLBCL subtype responsive to bortezomib, QALY gain was 0.2465 at a cost saving of GBP 6175, resulting in a net monetary benefit of GBP 13,570. In a probabilistic sensitivity analysis using 1000 simulations, a testing strategy was superior to a treat all with R-CHOP strategy in 81% of the simulations and with a cost saving in 92% assuming a cost price of zero.</p><h3>Conclusions</h3><p>Our estimates show that the combined test has a high probability of being cost effective. There is good quality evidence for the benefit of subtyping DLBCL but the evidence on the number of patients reclassified to or from BL and PMBCL and the impact of a more precise diagnosis and the cost of treatment is weak. The developers can use the price estimate to inform a return on investment calculations. Evidence will be required of how well the TempO-Seq<sup>®</sup> technology performs compared to the testing GEP technology used for subtyping in the recent clinical trial. For BL and PMBCL elements of the test, evidence would be required of the number of patients reclassified and improved costing information would be useful. The diagnostic and therapeutic environment in haematological malignancies is fast moving, which increases the risk for developers of diagnostic tests.</p></div>\",\"PeriodicalId\":8065,\"journal\":{\"name\":\"Applied Health Economics and Health Policy\",\"volume\":\"22 2\",\"pages\":\"243 - 254\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2023-11-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Applied Health Economics and Health Policy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://link.springer.com/article/10.1007/s40258-023-00845-1\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ECONOMICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Applied Health Economics and Health Policy","FirstCategoryId":"3","ListUrlMain":"https://link.springer.com/article/10.1007/s40258-023-00845-1","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ECONOMICS","Score":null,"Total":0}
Adding a Gene Expression Profile Test to Aid Differential Diagnosis and Treatment in Aggressive Large B-Cell Lymphoma: An Early Exploratory Economic Evaluation
Background and Objective
Adding gene expression profiles (GEPs) to the current diagnostic work-up of aggressive large B-cell lymphomas may lead to the reclassification of patients, treatment changes and improved outcomes. A GEP test is in development using TempO-Seq® technology to distinguish Burkitt lymphoma (BL) and primary mediastinal large B-cell lymphoma (PMBCL) from diffuse large B-cell lymphoma (DLBCL), and to classify patients with DLBLC and to predict the benefit of (e.g.) adding bortezomib to R-CHOP therapy (RB-CHOP). This study aims to estimate the potential impact of a GEP test on costs and health outcomes to inform pricing and evidence generation strategies.
Methods
Three decision models were developed comparing diagnostic strategies with and without GEP signatures over a lifetime horizon using a UK health and social care perspective. Inputs were taken from a recent clinical trial, literature and expert opinion. We estimated the maximum price of the test using a threshold of Great Britain Pound (GBP) 30,000 per quality-adjusted life-year (QALY). Sensitivity analyses were conducted.
Results
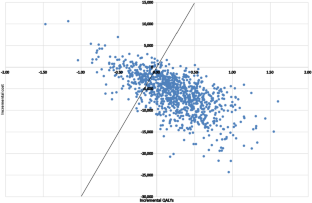
The estimated maximum threshold price for a combined test to be cost effective is GBP 15,352. At base-case values, the BL signature delivers QALY gains of 0.054 at an additional cost of GBP 275. This results in a net monetary benefit at a threshold of GBP 30,000 per QALY of GBP 1345. For PMBCL, the QALY gain was 0.0011 at a cost saving of GBP 406 and the net monetary benefit was GBP 437. The hazard ratio for the impact of treating BL less intensively must be at least 1.2 for a positive net monetary benefit. For identifying patients with the DLBCL subtype responsive to bortezomib, QALY gain was 0.2465 at a cost saving of GBP 6175, resulting in a net monetary benefit of GBP 13,570. In a probabilistic sensitivity analysis using 1000 simulations, a testing strategy was superior to a treat all with R-CHOP strategy in 81% of the simulations and with a cost saving in 92% assuming a cost price of zero.
Conclusions
Our estimates show that the combined test has a high probability of being cost effective. There is good quality evidence for the benefit of subtyping DLBCL but the evidence on the number of patients reclassified to or from BL and PMBCL and the impact of a more precise diagnosis and the cost of treatment is weak. The developers can use the price estimate to inform a return on investment calculations. Evidence will be required of how well the TempO-Seq® technology performs compared to the testing GEP technology used for subtyping in the recent clinical trial. For BL and PMBCL elements of the test, evidence would be required of the number of patients reclassified and improved costing information would be useful. The diagnostic and therapeutic environment in haematological malignancies is fast moving, which increases the risk for developers of diagnostic tests.
期刊介绍:
Applied Health Economics and Health Policy provides timely publication of cutting-edge research and expert opinion from this increasingly important field, making it a vital resource for payers, providers and researchers alike. The journal includes high quality economic research and reviews of all aspects of healthcare from various perspectives and countries, designed to communicate the latest applied information in health economics and health policy.
While emphasis is placed on information with practical applications, a strong basis of underlying scientific rigor is maintained.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


