{"title":"eb病毒与自身免疫:迫切需要有效的预防和治疗策略。","authors":"Piotr Rzymski, Agnieszka Szuster-Ciesielska","doi":"10.5114/reum/171506","DOIUrl":null,"url":null,"abstract":"Epstein-Barr virus (EBV), belonging to the family Orthoherpesviridae (subfamily Gammaherpesvirinae, genus Lymphocryptovirus), is a ubiquitous human pathogen with a 170 kilobase double-stranded DNA genome closed within an icosahedral capsid surrounded by a protein layer called the tegument and enclosed by a lipid envelope containing glycoproteins with high expression of gp350 and gp220 [1]. The tegument helps the virus replication and evasion of the cell’s immune response. Epstein-Barr virus is well-adapted to humans, its only known host, and primarily targets B cells due to their expression of CD21, the principal entry receptor for the virus. However, it can also infect epithelial cells by utilizing the ephrin receptor A2. Following acute infection, EBV persists in a latent state, causing life-long infection. Developing latency requires evasion of the immune response, which EBV achieves through blocking the expression of interferon genes, inhibiting complement activation, inactivating the cytotoxic functions of CD8+ lymphocytes, and inhibiting the host MHC class I antigen processing and presentation pathway [2]. During latency, the EBV genome usually persists in cell nuclei in the form of the multicopy, circular episome that associates with chromosomes during mitosis and is replicated by host DNA polymerase during the S phase. Different latent forms of EBV, varying in the transcriptional profile of non-coding RNAs and protein-coding mRNAs, have been identified (Fig. 1). Under conditions of altered cell-mediated immunity (induced by, e.g., stress, infections, immunosuppression), EBV reactivation can occur and not only lead to the onset of clinical symptoms and the virus becoming contagious but may also play a role in the pathogenesis of various diseases [3]. Epstein-Barr virus, which spreads most commonly by saliva, infects 90–95% of the world’s human population, but such a high prevalence does not justify disregarding it as a significant pathogen. Firstly, EBV is a causative agent of infectious mononucleosis, most commonly affecting children, adolescents, and young adults [4]. Secondly, it is the leading cause of post-transplant lymphoproliferative disease [4]. Thirdly, it has been classified as a group 1 carcinogen, implicated in the etiology of Burkitt’s lymphoma, Hodgkin’s disease, nasopharyngeal carcinoma, some T cell lymphomas, and selected cancers of the stomach and smooth muscle (Fig. 1), and is responsible for 240,000– 358,000 new cancer cases and 138,000–209,000 cancer-related deaths annually [5]. Epstein-Barr virus infection, particularly its reactivations, has also been implied in the autoimmune processes, acting as a trigger and/or a driver of selected autoimmune diseases (Table I). Further research is pivotal to elucidate genetic and environmental factors contributing to EBV-associated autoimmune effects [6]. The links between EBV infection and autoimmunity are continuously being explored, as evidenced by the increasing number of peer-reviewed articles focusing on such associations. As of August 2023, 1,772 articles searchable in the PubMed database with the key words “Epstein-Barr virus” and “autoimmunity” were identified, among which 49% had been published since 2010. In general, there are three main routes through which autoimmunity may be initiated in response to viral infection:","PeriodicalId":21312,"journal":{"name":"Reumatologia","volume":"61 5","pages":"327-330"},"PeriodicalIF":1.7000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10634406/pdf/","citationCount":"0","resultStr":"{\"title\":\"Epstein-Barr virus and autoimmunity: effective preventive and therapeutic strategies are urgently needed.\",\"authors\":\"Piotr Rzymski, Agnieszka Szuster-Ciesielska\",\"doi\":\"10.5114/reum/171506\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"Epstein-Barr virus (EBV), belonging to the family Orthoherpesviridae (subfamily Gammaherpesvirinae, genus Lymphocryptovirus), is a ubiquitous human pathogen with a 170 kilobase double-stranded DNA genome closed within an icosahedral capsid surrounded by a protein layer called the tegument and enclosed by a lipid envelope containing glycoproteins with high expression of gp350 and gp220 [1]. The tegument helps the virus replication and evasion of the cell’s immune response. Epstein-Barr virus is well-adapted to humans, its only known host, and primarily targets B cells due to their expression of CD21, the principal entry receptor for the virus. However, it can also infect epithelial cells by utilizing the ephrin receptor A2. Following acute infection, EBV persists in a latent state, causing life-long infection. Developing latency requires evasion of the immune response, which EBV achieves through blocking the expression of interferon genes, inhibiting complement activation, inactivating the cytotoxic functions of CD8+ lymphocytes, and inhibiting the host MHC class I antigen processing and presentation pathway [2]. During latency, the EBV genome usually persists in cell nuclei in the form of the multicopy, circular episome that associates with chromosomes during mitosis and is replicated by host DNA polymerase during the S phase. Different latent forms of EBV, varying in the transcriptional profile of non-coding RNAs and protein-coding mRNAs, have been identified (Fig. 1). Under conditions of altered cell-mediated immunity (induced by, e.g., stress, infections, immunosuppression), EBV reactivation can occur and not only lead to the onset of clinical symptoms and the virus becoming contagious but may also play a role in the pathogenesis of various diseases [3]. Epstein-Barr virus, which spreads most commonly by saliva, infects 90–95% of the world’s human population, but such a high prevalence does not justify disregarding it as a significant pathogen. Firstly, EBV is a causative agent of infectious mononucleosis, most commonly affecting children, adolescents, and young adults [4]. Secondly, it is the leading cause of post-transplant lymphoproliferative disease [4]. Thirdly, it has been classified as a group 1 carcinogen, implicated in the etiology of Burkitt’s lymphoma, Hodgkin’s disease, nasopharyngeal carcinoma, some T cell lymphomas, and selected cancers of the stomach and smooth muscle (Fig. 1), and is responsible for 240,000– 358,000 new cancer cases and 138,000–209,000 cancer-related deaths annually [5]. Epstein-Barr virus infection, particularly its reactivations, has also been implied in the autoimmune processes, acting as a trigger and/or a driver of selected autoimmune diseases (Table I). Further research is pivotal to elucidate genetic and environmental factors contributing to EBV-associated autoimmune effects [6]. The links between EBV infection and autoimmunity are continuously being explored, as evidenced by the increasing number of peer-reviewed articles focusing on such associations. As of August 2023, 1,772 articles searchable in the PubMed database with the key words “Epstein-Barr virus” and “autoimmunity” were identified, among which 49% had been published since 2010. In general, there are three main routes through which autoimmunity may be initiated in response to viral infection:\",\"PeriodicalId\":21312,\"journal\":{\"name\":\"Reumatologia\",\"volume\":\"61 5\",\"pages\":\"327-330\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10634406/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Reumatologia\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5114/reum/171506\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/10/10 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"RHEUMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Reumatologia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5114/reum/171506","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/10/10 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
Epstein-Barr virus and autoimmunity: effective preventive and therapeutic strategies are urgently needed.
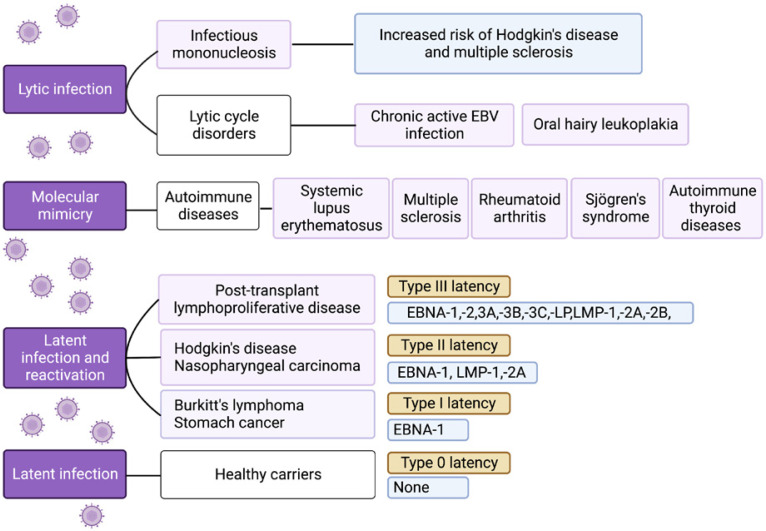
Epstein-Barr virus (EBV), belonging to the family Orthoherpesviridae (subfamily Gammaherpesvirinae, genus Lymphocryptovirus), is a ubiquitous human pathogen with a 170 kilobase double-stranded DNA genome closed within an icosahedral capsid surrounded by a protein layer called the tegument and enclosed by a lipid envelope containing glycoproteins with high expression of gp350 and gp220 [1]. The tegument helps the virus replication and evasion of the cell’s immune response. Epstein-Barr virus is well-adapted to humans, its only known host, and primarily targets B cells due to their expression of CD21, the principal entry receptor for the virus. However, it can also infect epithelial cells by utilizing the ephrin receptor A2. Following acute infection, EBV persists in a latent state, causing life-long infection. Developing latency requires evasion of the immune response, which EBV achieves through blocking the expression of interferon genes, inhibiting complement activation, inactivating the cytotoxic functions of CD8+ lymphocytes, and inhibiting the host MHC class I antigen processing and presentation pathway [2]. During latency, the EBV genome usually persists in cell nuclei in the form of the multicopy, circular episome that associates with chromosomes during mitosis and is replicated by host DNA polymerase during the S phase. Different latent forms of EBV, varying in the transcriptional profile of non-coding RNAs and protein-coding mRNAs, have been identified (Fig. 1). Under conditions of altered cell-mediated immunity (induced by, e.g., stress, infections, immunosuppression), EBV reactivation can occur and not only lead to the onset of clinical symptoms and the virus becoming contagious but may also play a role in the pathogenesis of various diseases [3]. Epstein-Barr virus, which spreads most commonly by saliva, infects 90–95% of the world’s human population, but such a high prevalence does not justify disregarding it as a significant pathogen. Firstly, EBV is a causative agent of infectious mononucleosis, most commonly affecting children, adolescents, and young adults [4]. Secondly, it is the leading cause of post-transplant lymphoproliferative disease [4]. Thirdly, it has been classified as a group 1 carcinogen, implicated in the etiology of Burkitt’s lymphoma, Hodgkin’s disease, nasopharyngeal carcinoma, some T cell lymphomas, and selected cancers of the stomach and smooth muscle (Fig. 1), and is responsible for 240,000– 358,000 new cancer cases and 138,000–209,000 cancer-related deaths annually [5]. Epstein-Barr virus infection, particularly its reactivations, has also been implied in the autoimmune processes, acting as a trigger and/or a driver of selected autoimmune diseases (Table I). Further research is pivotal to elucidate genetic and environmental factors contributing to EBV-associated autoimmune effects [6]. The links between EBV infection and autoimmunity are continuously being explored, as evidenced by the increasing number of peer-reviewed articles focusing on such associations. As of August 2023, 1,772 articles searchable in the PubMed database with the key words “Epstein-Barr virus” and “autoimmunity” were identified, among which 49% had been published since 2010. In general, there are three main routes through which autoimmunity may be initiated in response to viral infection:

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


