Michiko Nakaoka, Hideyuki Chiba, Mikio Kobayashi, Naoya Okada, Jun Arimoto, Jun Tachikawa, Keiichi Ashikari, Hiroki Kuwabara
{"title":"锯齿状息肉病综合征患者内镜控制的可行性和安全性。","authors":"Michiko Nakaoka, Hideyuki Chiba, Mikio Kobayashi, Naoya Okada, Jun Arimoto, Jun Tachikawa, Keiichi Ashikari, Hiroki Kuwabara","doi":"10.1159/000534968","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Despite advances in endoscopic treatment, patients with serrated polyposis syndrome (SPS) occasionally require surgery due to numerous or unresectable polyps, recurrence, and treatment-related adverse events.</p><p><strong>Methods: </strong>We retrospectively evaluated 43 patients with SPS undergoing diagnosis and treatment at Omori Red Cross Hospital from 2011 to 2022. Resection of all polyps ≥3 mm in size was planned during the clearing phase; endoscopic control was defined as complete, endoscopic polyp removal. During the surveillance phase, patients underwent annual colonoscopy and resection of newly detected polyps ≥3 mm in size.</p><p><strong>Results: </strong>Thirty-eight patients (88%) achieved endoscopic control, two (5%) required surgery after endoscopic treatment because of colorectal cancer (CRC), and three (7%) have not yet achieved endoscopic control and are planning treatment. Endoscopic control was achieved with a median of four colonoscopies at 8 months. Ten polyps (median value) were resected per patient during the clearing phase. Three polyps ≥50 mm in size, six located in the appendiceal orifice, and seven with severe fibrosis could be resected by endoscopic submucosal dissection (ESD). All patients underwent treatment with a combination of cold snare polypectomy (CSP), endoscopic mucosal resection/hot polypectomy, and/or ESD. No case required surgery due to difficulty with endoscopic treatment. Delayed bleeding was observed in 2 cases (0.3%). Twenty-one patients underwent colonoscopies during the surveillance phase. Fifty-three polyps were resected using CSP; no CRC, sessile serrated lesions with dysplasia, or advanced adenoma were detected.</p><p><strong>Conclusion: </strong>SPS can be effectively, efficiently, and safely controlled with appropriate endoscopic management.</p>","PeriodicalId":11294,"journal":{"name":"Digestive Diseases","volume":" ","pages":"31-40"},"PeriodicalIF":2.1000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10836738/pdf/","citationCount":"0","resultStr":"{\"title\":\"Feasibility and Safety of Endoscopic Control for Patients with Serrated Polyposis Syndrome.\",\"authors\":\"Michiko Nakaoka, Hideyuki Chiba, Mikio Kobayashi, Naoya Okada, Jun Arimoto, Jun Tachikawa, Keiichi Ashikari, Hiroki Kuwabara\",\"doi\":\"10.1159/000534968\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Despite advances in endoscopic treatment, patients with serrated polyposis syndrome (SPS) occasionally require surgery due to numerous or unresectable polyps, recurrence, and treatment-related adverse events.</p><p><strong>Methods: </strong>We retrospectively evaluated 43 patients with SPS undergoing diagnosis and treatment at Omori Red Cross Hospital from 2011 to 2022. Resection of all polyps ≥3 mm in size was planned during the clearing phase; endoscopic control was defined as complete, endoscopic polyp removal. During the surveillance phase, patients underwent annual colonoscopy and resection of newly detected polyps ≥3 mm in size.</p><p><strong>Results: </strong>Thirty-eight patients (88%) achieved endoscopic control, two (5%) required surgery after endoscopic treatment because of colorectal cancer (CRC), and three (7%) have not yet achieved endoscopic control and are planning treatment. Endoscopic control was achieved with a median of four colonoscopies at 8 months. Ten polyps (median value) were resected per patient during the clearing phase. Three polyps ≥50 mm in size, six located in the appendiceal orifice, and seven with severe fibrosis could be resected by endoscopic submucosal dissection (ESD). All patients underwent treatment with a combination of cold snare polypectomy (CSP), endoscopic mucosal resection/hot polypectomy, and/or ESD. No case required surgery due to difficulty with endoscopic treatment. Delayed bleeding was observed in 2 cases (0.3%). Twenty-one patients underwent colonoscopies during the surveillance phase. Fifty-three polyps were resected using CSP; no CRC, sessile serrated lesions with dysplasia, or advanced adenoma were detected.</p><p><strong>Conclusion: </strong>SPS can be effectively, efficiently, and safely controlled with appropriate endoscopic management.</p>\",\"PeriodicalId\":11294,\"journal\":{\"name\":\"Digestive Diseases\",\"volume\":\" \",\"pages\":\"31-40\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2024-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10836738/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Digestive Diseases\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1159/000534968\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/11/15 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Digestive Diseases","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1159/000534968","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/11/15 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Feasibility and Safety of Endoscopic Control for Patients with Serrated Polyposis Syndrome.
Introduction: Despite advances in endoscopic treatment, patients with serrated polyposis syndrome (SPS) occasionally require surgery due to numerous or unresectable polyps, recurrence, and treatment-related adverse events.
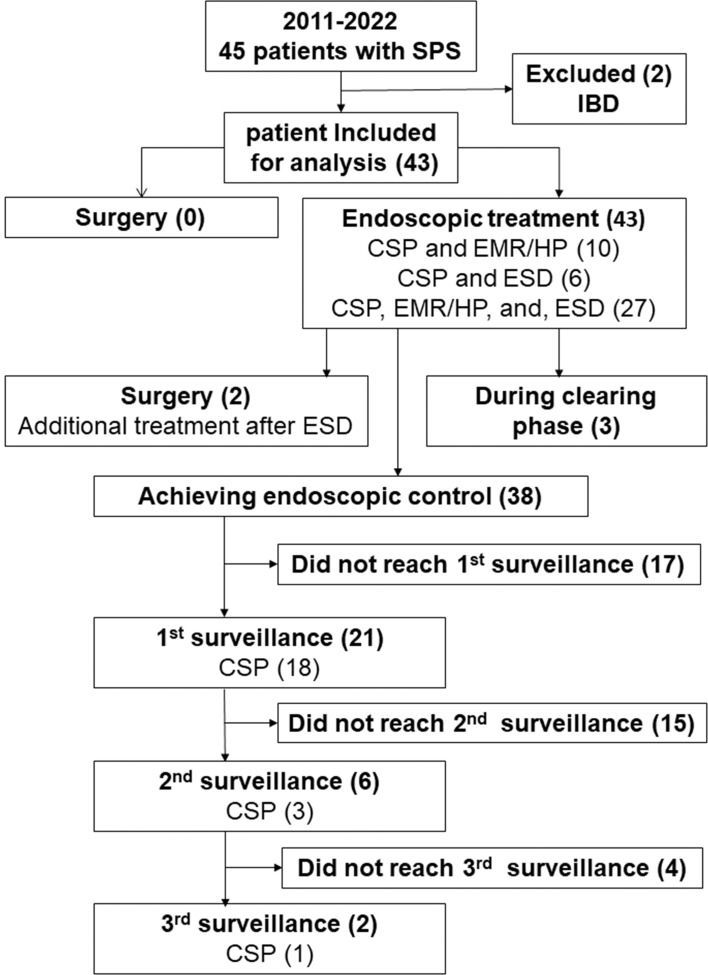
Methods: We retrospectively evaluated 43 patients with SPS undergoing diagnosis and treatment at Omori Red Cross Hospital from 2011 to 2022. Resection of all polyps ≥3 mm in size was planned during the clearing phase; endoscopic control was defined as complete, endoscopic polyp removal. During the surveillance phase, patients underwent annual colonoscopy and resection of newly detected polyps ≥3 mm in size.
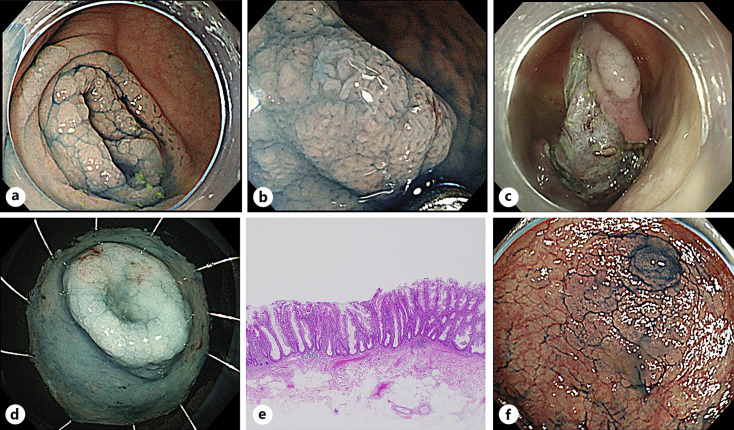
Results: Thirty-eight patients (88%) achieved endoscopic control, two (5%) required surgery after endoscopic treatment because of colorectal cancer (CRC), and three (7%) have not yet achieved endoscopic control and are planning treatment. Endoscopic control was achieved with a median of four colonoscopies at 8 months. Ten polyps (median value) were resected per patient during the clearing phase. Three polyps ≥50 mm in size, six located in the appendiceal orifice, and seven with severe fibrosis could be resected by endoscopic submucosal dissection (ESD). All patients underwent treatment with a combination of cold snare polypectomy (CSP), endoscopic mucosal resection/hot polypectomy, and/or ESD. No case required surgery due to difficulty with endoscopic treatment. Delayed bleeding was observed in 2 cases (0.3%). Twenty-one patients underwent colonoscopies during the surveillance phase. Fifty-three polyps were resected using CSP; no CRC, sessile serrated lesions with dysplasia, or advanced adenoma were detected.
Conclusion: SPS can be effectively, efficiently, and safely controlled with appropriate endoscopic management.
期刊介绍:
Each issue of this journal is dedicated to a special topic of current interest, covering both clinical and basic science topics in gastrointestinal function and disorders. The contents of each issue are comprehensive and reflect the state of the art, featuring editorials, reviews, mini reviews and original papers. These individual contributions encompass a variety of disciplines including all fields of gastroenterology. ''Digestive Diseases'' bridges the communication gap between advances made in the academic setting and their application in patient care. The journal is a valuable service for clinicians, specialists and physicians-in-training.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


