Louise V Bell, Sarah F Fitzgerald, David Flusk, Patricia A Poulin, Joshua A Rash
{"title":"在COVID-19出现之前,北美医疗保健提供者对阿片类药物治疗慢性非癌性疼痛的知识、信念和态度:对定性研究的系统回顾。","authors":"Louise V Bell, Sarah F Fitzgerald, David Flusk, Patricia A Poulin, Joshua A Rash","doi":"10.1080/24740527.2022.2156331","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Balance between benefits and harms of using opioids for the management of chronic noncancer pain (CNCP) must be carefully considered on a case-by-case basis. There is no one-size-fits-all approach that can be executed by prescribers and clinicians when considering this therapy.</p><p><strong>Aim: </strong>The aim of this study was to identify barriers and facilitators for prescribing opioids for CNCP through a systematic review of qualitative literature.</p><p><strong>Methods: </strong>Six databases were searched from inception to June 2019 for qualitative studies reporting on provider knowledge, attitudes, beliefs, or practices pertaining to prescribing opioids for CNCP in North America. Data were extracted, risk of bias was rated, and confidence in evidence was graded.</p><p><strong>Results: </strong>Twenty-seven studies reporting data from 599 health care providers were included. Ten themes emerged that influenced clinical decision making when prescribing opioids. Providers were more comfortable to prescribe opioids when (1) patients were actively engaged in pain self-management, (2) clear institutional prescribing policies were present and prescription drug monitoring programs were used, (3) long-standing relationships and strong therapeutic alliance were present, and (4) interprofessional supports were available. Factors that reduced likelihood of prescribing opioids included (1) uncertainty toward subjectivity of pain and efficacy of opioids, (2) concern for the patient (e.g., adverse effects) and community (i.e., diversion), (3) previous negative experiences (e.g., receiving threats), (4) difficulty enacting guidelines, and (5) organizational barriers (e.g., insufficient appointment duration and lengthy documentation).</p><p><strong>Conclusions: </strong>Understanding barriers and facilitators that influence opioid-prescribing practices offers insight into modifiable targets for interventions that can support providers in delivering care consistent with practice guidelines.</p>","PeriodicalId":53214,"journal":{"name":"Canadian Journal of Pain-Revue Canadienne de la Douleur","volume":"7 1","pages":"2156331"},"PeriodicalIF":2.1000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9980668/pdf/","citationCount":"1","resultStr":"{\"title\":\"Healthcare provider knowledge, beliefs, and attitudes regarding opioids for chronic non-cancer pain in North America prior to the emergence of COVID-19: A systematic review of qualitative research.\",\"authors\":\"Louise V Bell, Sarah F Fitzgerald, David Flusk, Patricia A Poulin, Joshua A Rash\",\"doi\":\"10.1080/24740527.2022.2156331\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Balance between benefits and harms of using opioids for the management of chronic noncancer pain (CNCP) must be carefully considered on a case-by-case basis. There is no one-size-fits-all approach that can be executed by prescribers and clinicians when considering this therapy.</p><p><strong>Aim: </strong>The aim of this study was to identify barriers and facilitators for prescribing opioids for CNCP through a systematic review of qualitative literature.</p><p><strong>Methods: </strong>Six databases were searched from inception to June 2019 for qualitative studies reporting on provider knowledge, attitudes, beliefs, or practices pertaining to prescribing opioids for CNCP in North America. Data were extracted, risk of bias was rated, and confidence in evidence was graded.</p><p><strong>Results: </strong>Twenty-seven studies reporting data from 599 health care providers were included. Ten themes emerged that influenced clinical decision making when prescribing opioids. Providers were more comfortable to prescribe opioids when (1) patients were actively engaged in pain self-management, (2) clear institutional prescribing policies were present and prescription drug monitoring programs were used, (3) long-standing relationships and strong therapeutic alliance were present, and (4) interprofessional supports were available. Factors that reduced likelihood of prescribing opioids included (1) uncertainty toward subjectivity of pain and efficacy of opioids, (2) concern for the patient (e.g., adverse effects) and community (i.e., diversion), (3) previous negative experiences (e.g., receiving threats), (4) difficulty enacting guidelines, and (5) organizational barriers (e.g., insufficient appointment duration and lengthy documentation).</p><p><strong>Conclusions: </strong>Understanding barriers and facilitators that influence opioid-prescribing practices offers insight into modifiable targets for interventions that can support providers in delivering care consistent with practice guidelines.</p>\",\"PeriodicalId\":53214,\"journal\":{\"name\":\"Canadian Journal of Pain-Revue Canadienne de la Douleur\",\"volume\":\"7 1\",\"pages\":\"2156331\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9980668/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Canadian Journal of Pain-Revue Canadienne de la Douleur\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1080/24740527.2022.2156331\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Pain-Revue Canadienne de la Douleur","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1080/24740527.2022.2156331","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Healthcare provider knowledge, beliefs, and attitudes regarding opioids for chronic non-cancer pain in North America prior to the emergence of COVID-19: A systematic review of qualitative research.
Background: Balance between benefits and harms of using opioids for the management of chronic noncancer pain (CNCP) must be carefully considered on a case-by-case basis. There is no one-size-fits-all approach that can be executed by prescribers and clinicians when considering this therapy.
Aim: The aim of this study was to identify barriers and facilitators for prescribing opioids for CNCP through a systematic review of qualitative literature.
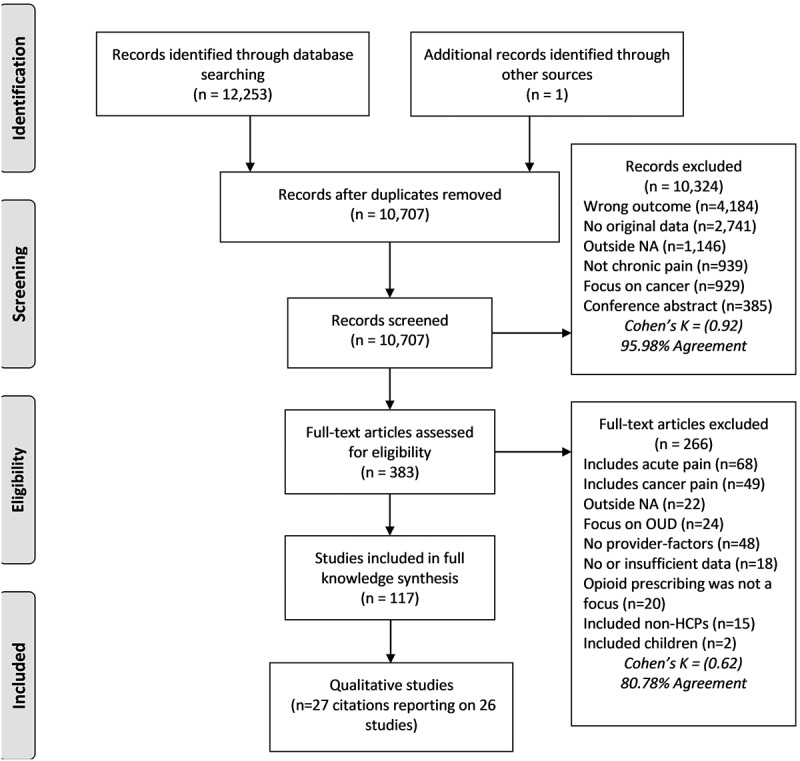
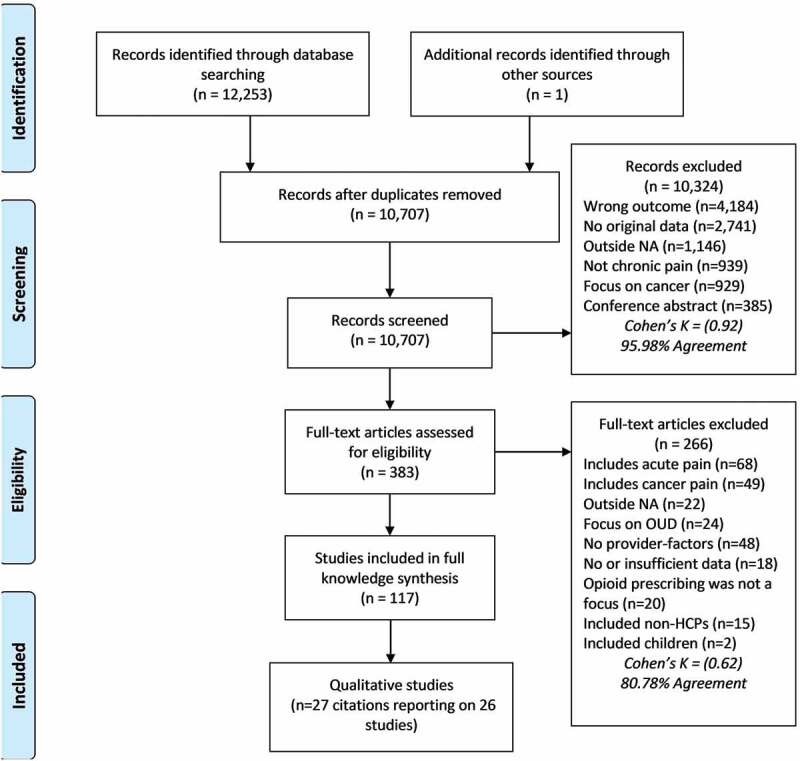
Methods: Six databases were searched from inception to June 2019 for qualitative studies reporting on provider knowledge, attitudes, beliefs, or practices pertaining to prescribing opioids for CNCP in North America. Data were extracted, risk of bias was rated, and confidence in evidence was graded.
Results: Twenty-seven studies reporting data from 599 health care providers were included. Ten themes emerged that influenced clinical decision making when prescribing opioids. Providers were more comfortable to prescribe opioids when (1) patients were actively engaged in pain self-management, (2) clear institutional prescribing policies were present and prescription drug monitoring programs were used, (3) long-standing relationships and strong therapeutic alliance were present, and (4) interprofessional supports were available. Factors that reduced likelihood of prescribing opioids included (1) uncertainty toward subjectivity of pain and efficacy of opioids, (2) concern for the patient (e.g., adverse effects) and community (i.e., diversion), (3) previous negative experiences (e.g., receiving threats), (4) difficulty enacting guidelines, and (5) organizational barriers (e.g., insufficient appointment duration and lengthy documentation).
Conclusions: Understanding barriers and facilitators that influence opioid-prescribing practices offers insight into modifiable targets for interventions that can support providers in delivering care consistent with practice guidelines.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


