Nomonde R Mvelase, Lindiwe P Cele, Ravesh Singh, Yeshnee Naidoo, Jennifer Giandhari, Eduan Wilkinson, Tulio de Oliveira, Khine Swe Swe-Han, Koleka P Mlisana
{"title":"南非程序化环境中基因型MTBDRplus检测遗漏的rpoB突变的后果","authors":"Nomonde R Mvelase, Lindiwe P Cele, Ravesh Singh, Yeshnee Naidoo, Jennifer Giandhari, Eduan Wilkinson, Tulio de Oliveira, Khine Swe Swe-Han, Koleka P Mlisana","doi":"10.4102/ajlm.v12i1.1975","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Rifampicin resistance missed by commercial rapid molecular assays but detected by phenotypic assays may lead to discordant susceptibility results and affect patient management.</p><p><strong>Objective: </strong>This study was conducted to evaluate the causes of rifampicin resistance missed by the GenoType MTBDR<i>plus</i> and its impact on the programmatic management of tuberculosis in KwaZulu-Natal, South Africa.</p><p><strong>Methods: </strong>We analysed routine tuberculosis programme data from January 2014 to December 2014 on isolates showing rifampicin susceptibility on the GenoType MTBDR<i>plus</i> assay but resistance on the phenotypic agar proportion method. Whole-genome sequencing was performed on a subset of these isolates.</p><p><strong>Results: </strong>Out of 505 patients with isoniazid mono-resistant tuberculosis on the MTBDR<i>plus</i>, 145 (28.7%) isolates showed both isoniazid and rifampicin resistance on the phenotypic assay. The mean time from MTBDR<i>plus</i> results to initiation of drug-resistant tuberculosis therapy was 93.7 days. 65.7% of the patients had received previous tuberculosis treatment. The most common mutations detected in the 36 sequenced isolates were I491F (16; 44.4%) and L452P (12; 33.3%). Among the 36 isolates, resistance to other anti-tuberculosis drugs was 69.4% for pyrazinamide, 83.3% for ethambutol, 69.4% for streptomycin, and 50% for ethionamide.</p><p><strong>Conclusion: </strong>Missed rifampicin resistance was mostly due to the I491F mutation located outside the MTBDR<i>plus</i> detection area and the L452P mutation, which was not included in the initial version 2 of the MTBDR<i>plus</i>. This led to substantial delays in the initiation of appropriate therapy. The previous tuberculosis treatment history and the high level of resistance to other anti-tuberculosis drugs suggest an accumulation of resistance.</p>","PeriodicalId":45412,"journal":{"name":"African Journal of Laboratory Medicine","volume":"12 1","pages":"1975"},"PeriodicalIF":1.2000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9982466/pdf/","citationCount":"3","resultStr":"{\"title\":\"Consequences of <i>rpoB</i> mutations missed by the GenoType MTBDR<i>plus</i> assay in a programmatic setting in South Africa.\",\"authors\":\"Nomonde R Mvelase, Lindiwe P Cele, Ravesh Singh, Yeshnee Naidoo, Jennifer Giandhari, Eduan Wilkinson, Tulio de Oliveira, Khine Swe Swe-Han, Koleka P Mlisana\",\"doi\":\"10.4102/ajlm.v12i1.1975\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Rifampicin resistance missed by commercial rapid molecular assays but detected by phenotypic assays may lead to discordant susceptibility results and affect patient management.</p><p><strong>Objective: </strong>This study was conducted to evaluate the causes of rifampicin resistance missed by the GenoType MTBDR<i>plus</i> and its impact on the programmatic management of tuberculosis in KwaZulu-Natal, South Africa.</p><p><strong>Methods: </strong>We analysed routine tuberculosis programme data from January 2014 to December 2014 on isolates showing rifampicin susceptibility on the GenoType MTBDR<i>plus</i> assay but resistance on the phenotypic agar proportion method. Whole-genome sequencing was performed on a subset of these isolates.</p><p><strong>Results: </strong>Out of 505 patients with isoniazid mono-resistant tuberculosis on the MTBDR<i>plus</i>, 145 (28.7%) isolates showed both isoniazid and rifampicin resistance on the phenotypic assay. The mean time from MTBDR<i>plus</i> results to initiation of drug-resistant tuberculosis therapy was 93.7 days. 65.7% of the patients had received previous tuberculosis treatment. The most common mutations detected in the 36 sequenced isolates were I491F (16; 44.4%) and L452P (12; 33.3%). Among the 36 isolates, resistance to other anti-tuberculosis drugs was 69.4% for pyrazinamide, 83.3% for ethambutol, 69.4% for streptomycin, and 50% for ethionamide.</p><p><strong>Conclusion: </strong>Missed rifampicin resistance was mostly due to the I491F mutation located outside the MTBDR<i>plus</i> detection area and the L452P mutation, which was not included in the initial version 2 of the MTBDR<i>plus</i>. This led to substantial delays in the initiation of appropriate therapy. The previous tuberculosis treatment history and the high level of resistance to other anti-tuberculosis drugs suggest an accumulation of resistance.</p>\",\"PeriodicalId\":45412,\"journal\":{\"name\":\"African Journal of Laboratory Medicine\",\"volume\":\"12 1\",\"pages\":\"1975\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9982466/pdf/\",\"citationCount\":\"3\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"African Journal of Laboratory Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4102/ajlm.v12i1.1975\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"MEDICINE, RESEARCH & EXPERIMENTAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"African Journal of Laboratory Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4102/ajlm.v12i1.1975","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
Consequences of rpoB mutations missed by the GenoType MTBDRplus assay in a programmatic setting in South Africa.
Background: Rifampicin resistance missed by commercial rapid molecular assays but detected by phenotypic assays may lead to discordant susceptibility results and affect patient management.
Objective: This study was conducted to evaluate the causes of rifampicin resistance missed by the GenoType MTBDRplus and its impact on the programmatic management of tuberculosis in KwaZulu-Natal, South Africa.
Methods: We analysed routine tuberculosis programme data from January 2014 to December 2014 on isolates showing rifampicin susceptibility on the GenoType MTBDRplus assay but resistance on the phenotypic agar proportion method. Whole-genome sequencing was performed on a subset of these isolates.
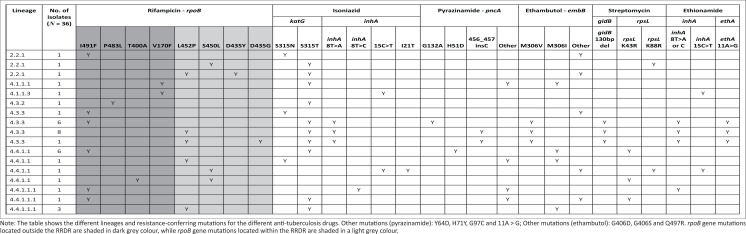
Results: Out of 505 patients with isoniazid mono-resistant tuberculosis on the MTBDRplus, 145 (28.7%) isolates showed both isoniazid and rifampicin resistance on the phenotypic assay. The mean time from MTBDRplus results to initiation of drug-resistant tuberculosis therapy was 93.7 days. 65.7% of the patients had received previous tuberculosis treatment. The most common mutations detected in the 36 sequenced isolates were I491F (16; 44.4%) and L452P (12; 33.3%). Among the 36 isolates, resistance to other anti-tuberculosis drugs was 69.4% for pyrazinamide, 83.3% for ethambutol, 69.4% for streptomycin, and 50% for ethionamide.
Conclusion: Missed rifampicin resistance was mostly due to the I491F mutation located outside the MTBDRplus detection area and the L452P mutation, which was not included in the initial version 2 of the MTBDRplus. This led to substantial delays in the initiation of appropriate therapy. The previous tuberculosis treatment history and the high level of resistance to other anti-tuberculosis drugs suggest an accumulation of resistance.
期刊介绍:
The African Journal of Laboratory Medicine, the official journal of ASLM, focuses on the role of the laboratory and its professionals in the clinical and public healthcare sectors,and is specifically based on an African frame of reference. Emphasis is on all aspects that promote and contribute to the laboratory medicine practices of Africa. This includes, amongst others: laboratories, biomedical scientists and clinicians, medical community, public health officials and policy makers, laboratory systems and policies (translation of laboratory knowledge, practices and technologies in clinical care), interfaces of laboratory with medical science, laboratory-based epidemiology, laboratory investigations, evidence-based effectiveness in real world (actual) settings.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


