Jon Cacicedo, Francisco Casquero, Arturo Navarro, Lorea Martinez-Indart, Olga Del Hoyo, Andere Frías, Roberto Ortiz de Zarate, David Büchser, Alfonso Gómez-Iturriaga, Iñigo San Miguel, Fernan Suarez, Adrian Barcena, Jose Luis López-Guerra
{"title":"以治愈为目的的老年非小细胞肺癌患者的治疗方法和预后因素的前瞻性多中心分析","authors":"Jon Cacicedo, Francisco Casquero, Arturo Navarro, Lorea Martinez-Indart, Olga Del Hoyo, Andere Frías, Roberto Ortiz de Zarate, David Büchser, Alfonso Gómez-Iturriaga, Iñigo San Miguel, Fernan Suarez, Adrian Barcena, Jose Luis López-Guerra","doi":"10.1259/bjro.20210058","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To analyse patterns of treatment with curative intent commonly used in elderly patients with locally advanced non-small-cell lung carcinoma (NSCLC) and predictive factors of overall survival in routine clinical practice.</p><p><strong>Methods: </strong>This multicentre prospective study included consecutive patients aged ≥65 years old diagnosed with NSCLC between February 2014 and January 2018. Inclusion criteria: age ≥65 years, stage IIIA/IIIB NSCLC. Treatment decisions were taken by a multidisciplinary committee. Kaplan-Meier curves and log-rank test were used to identify which clinical/treatment-associated variables, or pre-treatment quality of life (QOL) considering EORTC QLQ-C30 (and LC13 module) were predictive of overall survival.</p><p><strong>Results: </strong>A total of 139 patients were recruited. Median follow-up was 9.9 months (1.18-57.36 months) with a median survival of 14 months (range 11-17 months). In the group>75-year-old patients, the committee recommended chemotherapy and sequential radiotherapy (55.6%) or radiotherapy alone (22.2%), rather than surgery (3.7%) or concomitant radiochemotherapy (16.5%). However, in 65- to 75-year-old patients, surgery and concomitant radiochemotherapy were recommended in half of cases (p=0.003). Regarding multivariate analysis, the risk of death was higher in patients with pre-existing heart disease (p=0.002), low score for physical functioning (p=0.0001), symptoms of dysphagia (p=0,01), chest pain (p=0.001), and those not undergoing surgical treatment (p=0.024).</p><p><strong>Conclusions: </strong>Patients >75 years received more conservative treatments. Surgery improved survival and should be carefully considered, regardless of patient age. Comorbidities and poor baseline QOL are predictive of shorter survival.</p><p><strong>Advances in knowledge: </strong>Measuring these parameters before treatment may help us to define a population of frail patients with a poorer prognosis to facilitate decision making in clinical practice.</p>","PeriodicalId":72419,"journal":{"name":"BJR open","volume":"4 1","pages":"20210058"},"PeriodicalIF":0.0000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9459856/pdf/","citationCount":"2","resultStr":"{\"title\":\"Prospective multicentre analysis of the therapeutic approach and prognostic factors determining overall survival in elderly patients with non-small-cell lung carcinoma treated with curative intent.\",\"authors\":\"Jon Cacicedo, Francisco Casquero, Arturo Navarro, Lorea Martinez-Indart, Olga Del Hoyo, Andere Frías, Roberto Ortiz de Zarate, David Büchser, Alfonso Gómez-Iturriaga, Iñigo San Miguel, Fernan Suarez, Adrian Barcena, Jose Luis López-Guerra\",\"doi\":\"10.1259/bjro.20210058\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To analyse patterns of treatment with curative intent commonly used in elderly patients with locally advanced non-small-cell lung carcinoma (NSCLC) and predictive factors of overall survival in routine clinical practice.</p><p><strong>Methods: </strong>This multicentre prospective study included consecutive patients aged ≥65 years old diagnosed with NSCLC between February 2014 and January 2018. Inclusion criteria: age ≥65 years, stage IIIA/IIIB NSCLC. Treatment decisions were taken by a multidisciplinary committee. Kaplan-Meier curves and log-rank test were used to identify which clinical/treatment-associated variables, or pre-treatment quality of life (QOL) considering EORTC QLQ-C30 (and LC13 module) were predictive of overall survival.</p><p><strong>Results: </strong>A total of 139 patients were recruited. Median follow-up was 9.9 months (1.18-57.36 months) with a median survival of 14 months (range 11-17 months). In the group>75-year-old patients, the committee recommended chemotherapy and sequential radiotherapy (55.6%) or radiotherapy alone (22.2%), rather than surgery (3.7%) or concomitant radiochemotherapy (16.5%). However, in 65- to 75-year-old patients, surgery and concomitant radiochemotherapy were recommended in half of cases (p=0.003). Regarding multivariate analysis, the risk of death was higher in patients with pre-existing heart disease (p=0.002), low score for physical functioning (p=0.0001), symptoms of dysphagia (p=0,01), chest pain (p=0.001), and those not undergoing surgical treatment (p=0.024).</p><p><strong>Conclusions: </strong>Patients >75 years received more conservative treatments. Surgery improved survival and should be carefully considered, regardless of patient age. Comorbidities and poor baseline QOL are predictive of shorter survival.</p><p><strong>Advances in knowledge: </strong>Measuring these parameters before treatment may help us to define a population of frail patients with a poorer prognosis to facilitate decision making in clinical practice.</p>\",\"PeriodicalId\":72419,\"journal\":{\"name\":\"BJR open\",\"volume\":\"4 1\",\"pages\":\"20210058\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9459856/pdf/\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BJR open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1259/bjro.20210058\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BJR open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1259/bjro.20210058","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Prospective multicentre analysis of the therapeutic approach and prognostic factors determining overall survival in elderly patients with non-small-cell lung carcinoma treated with curative intent.
Objective: To analyse patterns of treatment with curative intent commonly used in elderly patients with locally advanced non-small-cell lung carcinoma (NSCLC) and predictive factors of overall survival in routine clinical practice.
Methods: This multicentre prospective study included consecutive patients aged ≥65 years old diagnosed with NSCLC between February 2014 and January 2018. Inclusion criteria: age ≥65 years, stage IIIA/IIIB NSCLC. Treatment decisions were taken by a multidisciplinary committee. Kaplan-Meier curves and log-rank test were used to identify which clinical/treatment-associated variables, or pre-treatment quality of life (QOL) considering EORTC QLQ-C30 (and LC13 module) were predictive of overall survival.
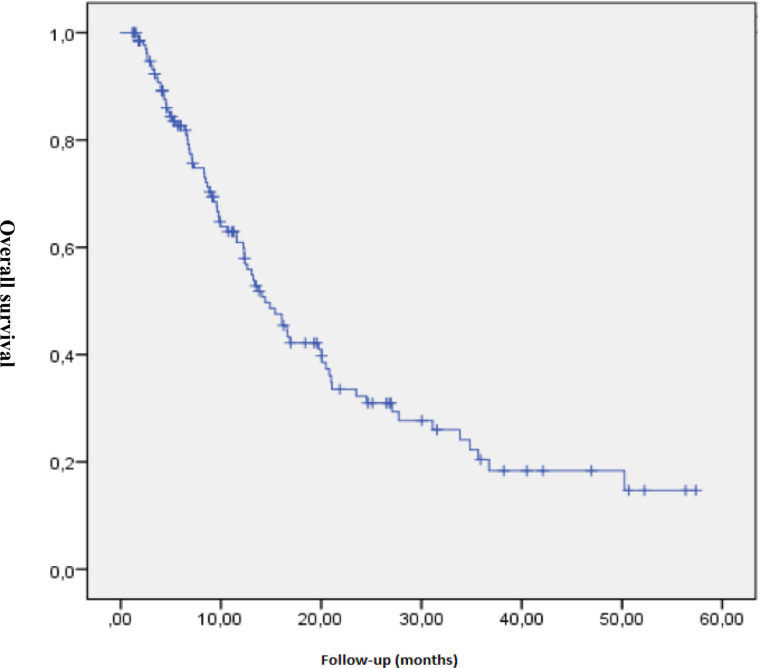
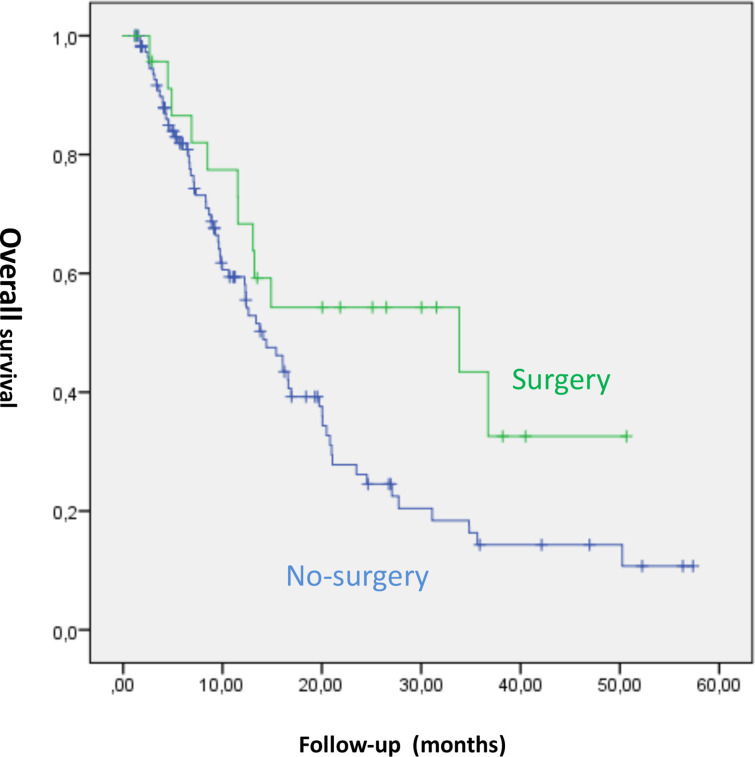
Results: A total of 139 patients were recruited. Median follow-up was 9.9 months (1.18-57.36 months) with a median survival of 14 months (range 11-17 months). In the group>75-year-old patients, the committee recommended chemotherapy and sequential radiotherapy (55.6%) or radiotherapy alone (22.2%), rather than surgery (3.7%) or concomitant radiochemotherapy (16.5%). However, in 65- to 75-year-old patients, surgery and concomitant radiochemotherapy were recommended in half of cases (p=0.003). Regarding multivariate analysis, the risk of death was higher in patients with pre-existing heart disease (p=0.002), low score for physical functioning (p=0.0001), symptoms of dysphagia (p=0,01), chest pain (p=0.001), and those not undergoing surgical treatment (p=0.024).
Conclusions: Patients >75 years received more conservative treatments. Surgery improved survival and should be carefully considered, regardless of patient age. Comorbidities and poor baseline QOL are predictive of shorter survival.
Advances in knowledge: Measuring these parameters before treatment may help us to define a population of frail patients with a poorer prognosis to facilitate decision making in clinical practice.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


