{"title":"住院心脏骤停患者的存活至出院率和良好的神经转归与性别、复苏时间和首次文献相关:一项系统荟萃分析","authors":"Afshin Goodarzi, Mahnaz Khatiban, Alireza Abdi, Khodayar Oshvandi","doi":"10.30476/BEAT.2022.92465.1307","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To investigate the relationship between outcomes and demographic-clinical variables in in-hospital cardiac arrest (IHCA).</p><p><strong>Methods: </strong>The Medline database was searched along with Google Scholar, Scopus, Web of Science, and Persian language database without time limitation until January 6<sup>th</sup>, 2020. The inclusion criteria included papers published in journals or presented in English and Persian congress that reported the IHCA outcomes based on the Utstein criterion. All the descriptive, cross-sectional, and cohort studies on CPR were covered based on inclusion and exclusion criteria. Primary checks covered titles and abstracts followed by a full-text check of the remaining papers from the first screening stage. Data analysis was done using comprehensive meta-analysis (CMA) software version 2.0. The finding's heterogeneity was checked using Q and Cochran tests with heterogeneity >50% and the random-effects model was used to estimate survival and favorable neurological outcome (FNO) in the analysis. To detect the publication bias of studies, the subgroup test, meta-regression test, sensitivity analysis test, funnel plot, and Eagger's regression test were used.</p><p><strong>Results: </strong>Survival to discharge was 19.1% (95% CI=16.8-21.7) and FNO in the survived to discharge cases was 68.1% (95% CI=55.8-78.3). Survival to discharge and FNO were notably higher in men, CPR duration <15min, and shockable dysrhythmias.</p><p><strong>Conclusion: </strong><b>IHCA</b> outcomes are poor in developing countries. The outcomes of IHCA in terms of gender were inconsistent with the result reported by other meta-analyses.</p>","PeriodicalId":9333,"journal":{"name":"Bulletin of emergency and trauma","volume":"10 4","pages":"141-156"},"PeriodicalIF":0.0000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/09/24/bet-10-141.PMC9758708.pdf","citationCount":"0","resultStr":"{\"title\":\"Survival to Discharge Rate and Favorable Neurological Outcome Related to Gender, Duration of Resuscitation and First Document of Patients In-Hospital Cardiac Arrest: A Systematic Meta-Analysis.\",\"authors\":\"Afshin Goodarzi, Mahnaz Khatiban, Alireza Abdi, Khodayar Oshvandi\",\"doi\":\"10.30476/BEAT.2022.92465.1307\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To investigate the relationship between outcomes and demographic-clinical variables in in-hospital cardiac arrest (IHCA).</p><p><strong>Methods: </strong>The Medline database was searched along with Google Scholar, Scopus, Web of Science, and Persian language database without time limitation until January 6<sup>th</sup>, 2020. The inclusion criteria included papers published in journals or presented in English and Persian congress that reported the IHCA outcomes based on the Utstein criterion. All the descriptive, cross-sectional, and cohort studies on CPR were covered based on inclusion and exclusion criteria. Primary checks covered titles and abstracts followed by a full-text check of the remaining papers from the first screening stage. Data analysis was done using comprehensive meta-analysis (CMA) software version 2.0. The finding's heterogeneity was checked using Q and Cochran tests with heterogeneity >50% and the random-effects model was used to estimate survival and favorable neurological outcome (FNO) in the analysis. To detect the publication bias of studies, the subgroup test, meta-regression test, sensitivity analysis test, funnel plot, and Eagger's regression test were used.</p><p><strong>Results: </strong>Survival to discharge was 19.1% (95% CI=16.8-21.7) and FNO in the survived to discharge cases was 68.1% (95% CI=55.8-78.3). Survival to discharge and FNO were notably higher in men, CPR duration <15min, and shockable dysrhythmias.</p><p><strong>Conclusion: </strong><b>IHCA</b> outcomes are poor in developing countries. The outcomes of IHCA in terms of gender were inconsistent with the result reported by other meta-analyses.</p>\",\"PeriodicalId\":9333,\"journal\":{\"name\":\"Bulletin of emergency and trauma\",\"volume\":\"10 4\",\"pages\":\"141-156\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/09/24/bet-10-141.PMC9758708.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Bulletin of emergency and trauma\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.30476/BEAT.2022.92465.1307\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Bulletin of emergency and trauma","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.30476/BEAT.2022.92465.1307","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Survival to Discharge Rate and Favorable Neurological Outcome Related to Gender, Duration of Resuscitation and First Document of Patients In-Hospital Cardiac Arrest: A Systematic Meta-Analysis.
Objective: To investigate the relationship between outcomes and demographic-clinical variables in in-hospital cardiac arrest (IHCA).
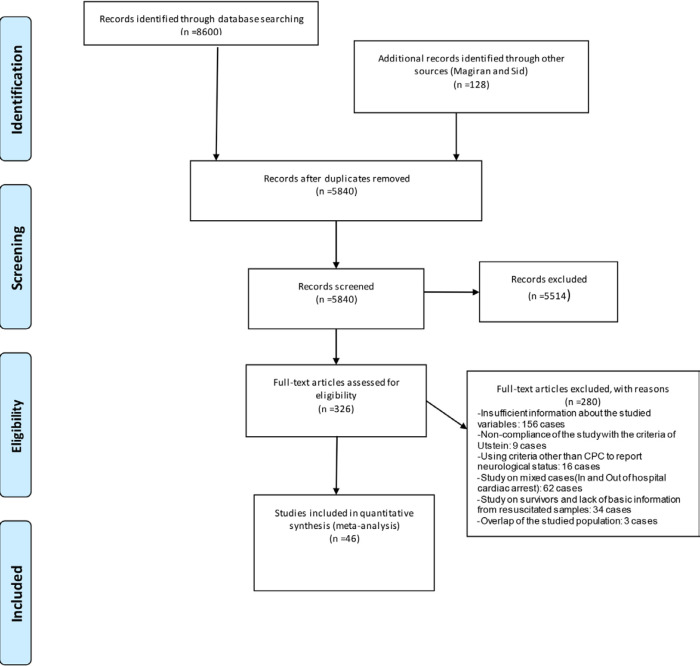
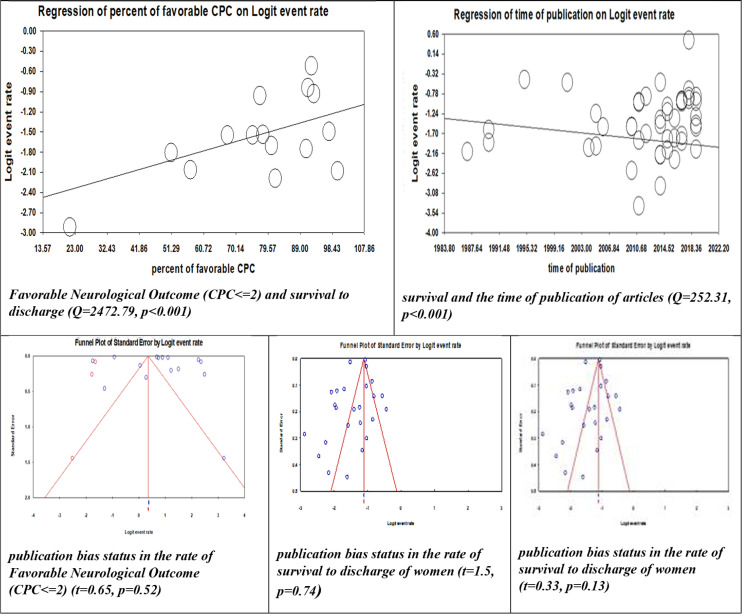
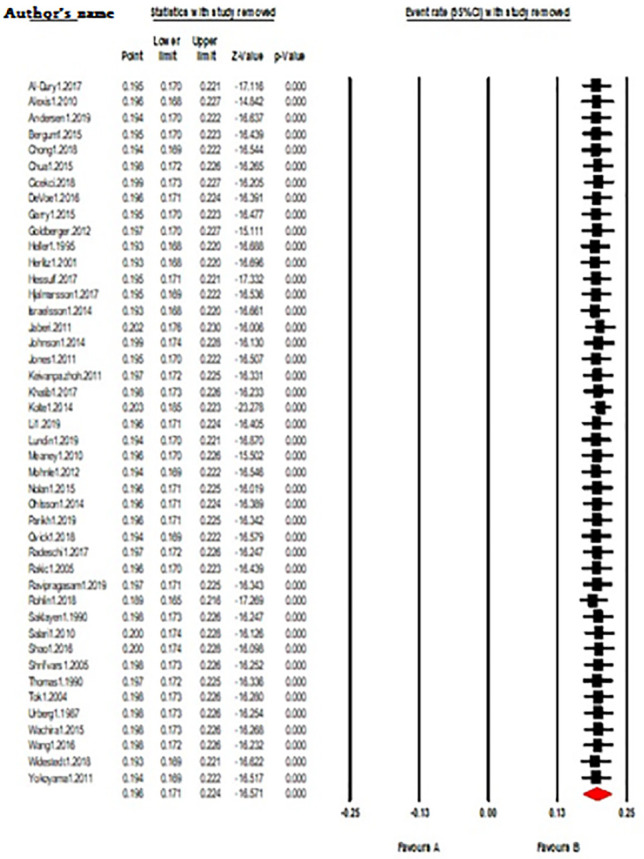
Methods: The Medline database was searched along with Google Scholar, Scopus, Web of Science, and Persian language database without time limitation until January 6th, 2020. The inclusion criteria included papers published in journals or presented in English and Persian congress that reported the IHCA outcomes based on the Utstein criterion. All the descriptive, cross-sectional, and cohort studies on CPR were covered based on inclusion and exclusion criteria. Primary checks covered titles and abstracts followed by a full-text check of the remaining papers from the first screening stage. Data analysis was done using comprehensive meta-analysis (CMA) software version 2.0. The finding's heterogeneity was checked using Q and Cochran tests with heterogeneity >50% and the random-effects model was used to estimate survival and favorable neurological outcome (FNO) in the analysis. To detect the publication bias of studies, the subgroup test, meta-regression test, sensitivity analysis test, funnel plot, and Eagger's regression test were used.
Results: Survival to discharge was 19.1% (95% CI=16.8-21.7) and FNO in the survived to discharge cases was 68.1% (95% CI=55.8-78.3). Survival to discharge and FNO were notably higher in men, CPR duration <15min, and shockable dysrhythmias.
Conclusion: IHCA outcomes are poor in developing countries. The outcomes of IHCA in terms of gender were inconsistent with the result reported by other meta-analyses.
期刊介绍:
BEAT: Bulletin of Emergency And Trauma is an international, peer-reviewed, quarterly journal coping with original research contributing to the field of emergency medicine and trauma. BEAT is the official journal of the Trauma Research Center (TRC) of Shiraz University of Medical Sciences (SUMS), Hungarian Trauma Society (HTS) and Lusitanian Association for Trauma and Emergency Surgery (ALTEC/LATES) aiming to be a publication of international repute that serves as a medium for dissemination and exchange of scientific knowledge in the emergency medicine and trauma. The aim of BEAT is to publish original research focusing on practicing and training of emergency medicine and trauma to publish peer-reviewed articles of current international interest in the form of original articles, brief communications, reviews, case reports, clinical images, and letters.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


