Haider Aldiwani, Michael D Nelson, Behzad Sharif, Janet Wei, T Jake Samuel, Nissi Suppogu, Odayme Quesada, Galen Cook-Wiens, Edward Gill, Lidia S Szczepaniak, Louise E J Thomson, Balaji Tamarappoo, Anum Asif, Chrisandra Shufelt, Daniel Berman, C Noel Bairey Merz
{"title":"心肌灌注减少在心肌缺血、无阻塞性冠状动脉疾病和射血分数保留型心力衰竭患者中很常见:WISE-CVD 持续研究报告。","authors":"Haider Aldiwani, Michael D Nelson, Behzad Sharif, Janet Wei, T Jake Samuel, Nissi Suppogu, Odayme Quesada, Galen Cook-Wiens, Edward Gill, Lidia S Szczepaniak, Louise E J Thomson, Balaji Tamarappoo, Anum Asif, Chrisandra Shufelt, Daniel Berman, C Noel Bairey Merz","doi":"10.20517/2574-1209.2021.103","DOIUrl":null,"url":null,"abstract":"<p><strong>Aim: </strong>Women with evidence of ischemia and no obstructive coronary artery disease (INOCA) have an increased risk of major adverse cardiac events, including heart failure with preserved ejection fraction (HFpEF). To investigate potential links between INOCA and HFpEF, we examined pathophysiological findings present in both INOCA and HFpEF.</p><p><strong>Methods: </strong>We performed adenosine stress cardiac magnetic resonance imaging (CMRI) in 56 participants, including 35 women with suspected INOCA, 13 women with HFpEF, and 8 reference control women. Myocardial perfusion imaging was performed at rest and with vasodilator stress with intravenous adenosine. Myocardial perfusion reserve index was quantified as the ratio of the upslope of increase in myocardial contrast at stress <i>vs</i>. rest. All CMRI measures were quantified using CVI42 software (Circle Cardiovascular Imaging Inc). Statistical analysis was performed using linear regression models, Fisher's exact tests, ANOVA, or Kruskal-Wallis tests.</p><p><strong>Results: </strong>Age (<i>P</i> = 0.007), Body surface area (0.05) were higher in the HFpEF group. Left ventricular ejection fraction (<i>P</i> = 0.02) was lower among the INOCA and HFpEF groups than reference controls after age adjustment. In addition, there was a graded reduction in myocardial perfusion reserve index in HFpEF <i>vs</i>. INOCA <i>vs</i>. reference controls (1.5 ± 0.3, 1.8 ± 0.3, 1.9 ± 0.3, <i>P</i> = 0.02), which was attenuated with age-adjustment.</p><p><strong>Conclusion: </strong>Reduced myocardial perfusion reserve appears to be a common pathophysiologic feature in INOCA and HFpEF patients.</p>","PeriodicalId":75299,"journal":{"name":"Vessel plus","volume":"6 ","pages":""},"PeriodicalIF":0.7000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9278056/pdf/","citationCount":"0","resultStr":"{\"title\":\"Reduced myocardial perfusion is common among subjects with ischemia and no obstructive coronary artery disease and heart failure with preserved ejection fraction: a report from the WISE-CVD continuation study.\",\"authors\":\"Haider Aldiwani, Michael D Nelson, Behzad Sharif, Janet Wei, T Jake Samuel, Nissi Suppogu, Odayme Quesada, Galen Cook-Wiens, Edward Gill, Lidia S Szczepaniak, Louise E J Thomson, Balaji Tamarappoo, Anum Asif, Chrisandra Shufelt, Daniel Berman, C Noel Bairey Merz\",\"doi\":\"10.20517/2574-1209.2021.103\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aim: </strong>Women with evidence of ischemia and no obstructive coronary artery disease (INOCA) have an increased risk of major adverse cardiac events, including heart failure with preserved ejection fraction (HFpEF). To investigate potential links between INOCA and HFpEF, we examined pathophysiological findings present in both INOCA and HFpEF.</p><p><strong>Methods: </strong>We performed adenosine stress cardiac magnetic resonance imaging (CMRI) in 56 participants, including 35 women with suspected INOCA, 13 women with HFpEF, and 8 reference control women. Myocardial perfusion imaging was performed at rest and with vasodilator stress with intravenous adenosine. Myocardial perfusion reserve index was quantified as the ratio of the upslope of increase in myocardial contrast at stress <i>vs</i>. rest. All CMRI measures were quantified using CVI42 software (Circle Cardiovascular Imaging Inc). Statistical analysis was performed using linear regression models, Fisher's exact tests, ANOVA, or Kruskal-Wallis tests.</p><p><strong>Results: </strong>Age (<i>P</i> = 0.007), Body surface area (0.05) were higher in the HFpEF group. Left ventricular ejection fraction (<i>P</i> = 0.02) was lower among the INOCA and HFpEF groups than reference controls after age adjustment. In addition, there was a graded reduction in myocardial perfusion reserve index in HFpEF <i>vs</i>. INOCA <i>vs</i>. reference controls (1.5 ± 0.3, 1.8 ± 0.3, 1.9 ± 0.3, <i>P</i> = 0.02), which was attenuated with age-adjustment.</p><p><strong>Conclusion: </strong>Reduced myocardial perfusion reserve appears to be a common pathophysiologic feature in INOCA and HFpEF patients.</p>\",\"PeriodicalId\":75299,\"journal\":{\"name\":\"Vessel plus\",\"volume\":\"6 \",\"pages\":\"\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2022-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9278056/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Vessel plus\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.20517/2574-1209.2021.103\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/3/5 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Vessel plus","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.20517/2574-1209.2021.103","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/3/5 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Reduced myocardial perfusion is common among subjects with ischemia and no obstructive coronary artery disease and heart failure with preserved ejection fraction: a report from the WISE-CVD continuation study.
Aim: Women with evidence of ischemia and no obstructive coronary artery disease (INOCA) have an increased risk of major adverse cardiac events, including heart failure with preserved ejection fraction (HFpEF). To investigate potential links between INOCA and HFpEF, we examined pathophysiological findings present in both INOCA and HFpEF.
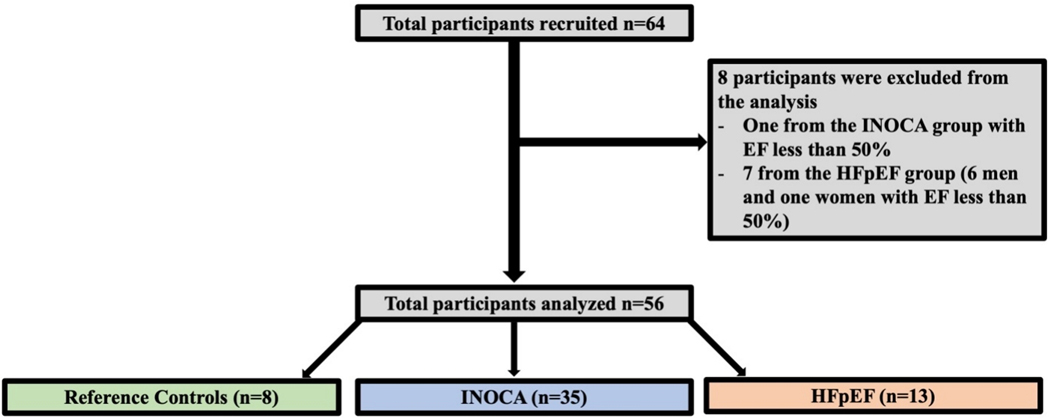
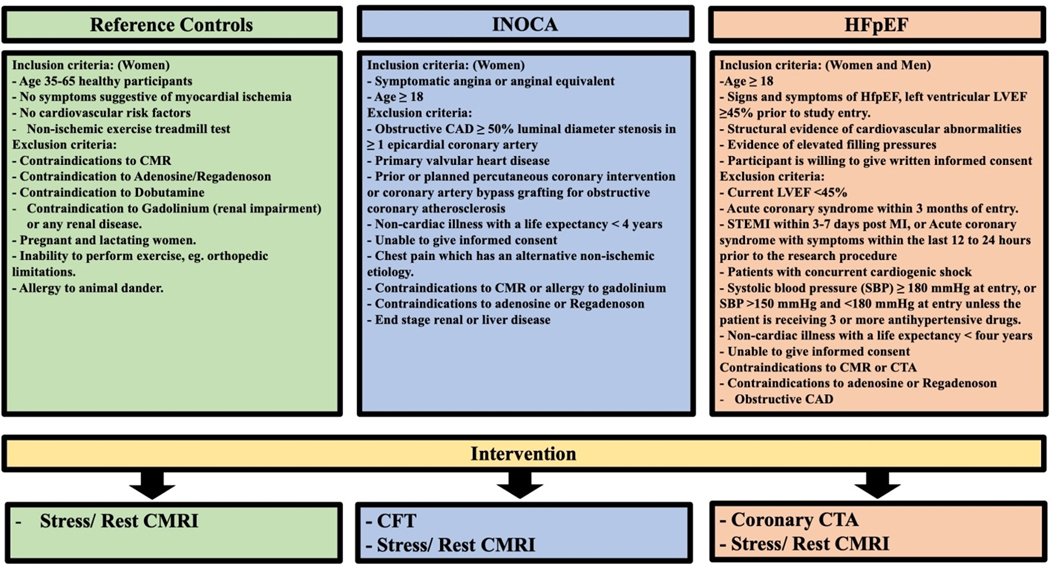
Methods: We performed adenosine stress cardiac magnetic resonance imaging (CMRI) in 56 participants, including 35 women with suspected INOCA, 13 women with HFpEF, and 8 reference control women. Myocardial perfusion imaging was performed at rest and with vasodilator stress with intravenous adenosine. Myocardial perfusion reserve index was quantified as the ratio of the upslope of increase in myocardial contrast at stress vs. rest. All CMRI measures were quantified using CVI42 software (Circle Cardiovascular Imaging Inc). Statistical analysis was performed using linear regression models, Fisher's exact tests, ANOVA, or Kruskal-Wallis tests.
Results: Age (P = 0.007), Body surface area (0.05) were higher in the HFpEF group. Left ventricular ejection fraction (P = 0.02) was lower among the INOCA and HFpEF groups than reference controls after age adjustment. In addition, there was a graded reduction in myocardial perfusion reserve index in HFpEF vs. INOCA vs. reference controls (1.5 ± 0.3, 1.8 ± 0.3, 1.9 ± 0.3, P = 0.02), which was attenuated with age-adjustment.
Conclusion: Reduced myocardial perfusion reserve appears to be a common pathophysiologic feature in INOCA and HFpEF patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


