Ahmed Badran, Saad Salman Ali, Tarek Ziad Arabi, Abdullaah Khaleel Hinkston, Abdullah Shaik, Mahmoud A Elshenawy, Dahish Ajarim
{"title":"吉西他滨诱导的B型乳腺癌患者肌炎1例报告。","authors":"Ahmed Badran, Saad Salman Ali, Tarek Ziad Arabi, Abdullaah Khaleel Hinkston, Abdullah Shaik, Mahmoud A Elshenawy, Dahish Ajarim","doi":"10.1177/11795476231156290","DOIUrl":null,"url":null,"abstract":"<p><p>Human epidermal growth factor receptor-positive breast cancer is an aggressive cancer which represents approximately a quarter of all breast cancers worldwide. Recent advances have led to the development of targeted therapies, such as trastuzumab (H), which have significantly improved prognosis. Such therapies are currently used alongside other chemotherapeutic agents, such as paclitaxel (P) and gemcitabine (G). The most common side effects of PGH combination therapy include thrombocytopenia and anemias. However, there have been no previous reports of myositis resulting from this combination. We report the case of a 54-year-old metastatic breast cancer patient on PGH therapy who developed muscle weakness. The patient was initially treated with trastuzumab, pertuzumab, and paclitaxel. However, pertuzumab was changed to gemcitabine due to severe diarrhea. After the fourth cycle of PGH, the patient presented with muscle weakness and creatine kinase levels of up to 6755 U/L. Magnetic resonance imaging of the femur and pelvis revealed diffuse bilateral myositis, suggesting a diagnosis of gemcitabine-induced myositis. The patient was placed on intravenous fluids and corticosteroids, which resolved her condition. To our knowledge, this is the first report of gemcitabine-induced myositis in a breast cancer patient. Further studies are needed to determine the underlying mechanisms of gemcitabine-induced myositis and develop preventative measures.</p>","PeriodicalId":10357,"journal":{"name":"Clinical Medicine Insights. Case Reports","volume":"16 ","pages":"11795476231156290"},"PeriodicalIF":0.8000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/68/15/10.1177_11795476231156290.PMC9941597.pdf","citationCount":"1","resultStr":"{\"title\":\"Gemcitabine-Induced Myositis in a Luminal B Breast Cancer patient: A Case Report.\",\"authors\":\"Ahmed Badran, Saad Salman Ali, Tarek Ziad Arabi, Abdullaah Khaleel Hinkston, Abdullah Shaik, Mahmoud A Elshenawy, Dahish Ajarim\",\"doi\":\"10.1177/11795476231156290\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Human epidermal growth factor receptor-positive breast cancer is an aggressive cancer which represents approximately a quarter of all breast cancers worldwide. Recent advances have led to the development of targeted therapies, such as trastuzumab (H), which have significantly improved prognosis. Such therapies are currently used alongside other chemotherapeutic agents, such as paclitaxel (P) and gemcitabine (G). The most common side effects of PGH combination therapy include thrombocytopenia and anemias. However, there have been no previous reports of myositis resulting from this combination. We report the case of a 54-year-old metastatic breast cancer patient on PGH therapy who developed muscle weakness. The patient was initially treated with trastuzumab, pertuzumab, and paclitaxel. However, pertuzumab was changed to gemcitabine due to severe diarrhea. After the fourth cycle of PGH, the patient presented with muscle weakness and creatine kinase levels of up to 6755 U/L. Magnetic resonance imaging of the femur and pelvis revealed diffuse bilateral myositis, suggesting a diagnosis of gemcitabine-induced myositis. The patient was placed on intravenous fluids and corticosteroids, which resolved her condition. To our knowledge, this is the first report of gemcitabine-induced myositis in a breast cancer patient. Further studies are needed to determine the underlying mechanisms of gemcitabine-induced myositis and develop preventative measures.</p>\",\"PeriodicalId\":10357,\"journal\":{\"name\":\"Clinical Medicine Insights. Case Reports\",\"volume\":\"16 \",\"pages\":\"11795476231156290\"},\"PeriodicalIF\":0.8000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/68/15/10.1177_11795476231156290.PMC9941597.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Medicine Insights. Case Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/11795476231156290\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights. Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/11795476231156290","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Gemcitabine-Induced Myositis in a Luminal B Breast Cancer patient: A Case Report.
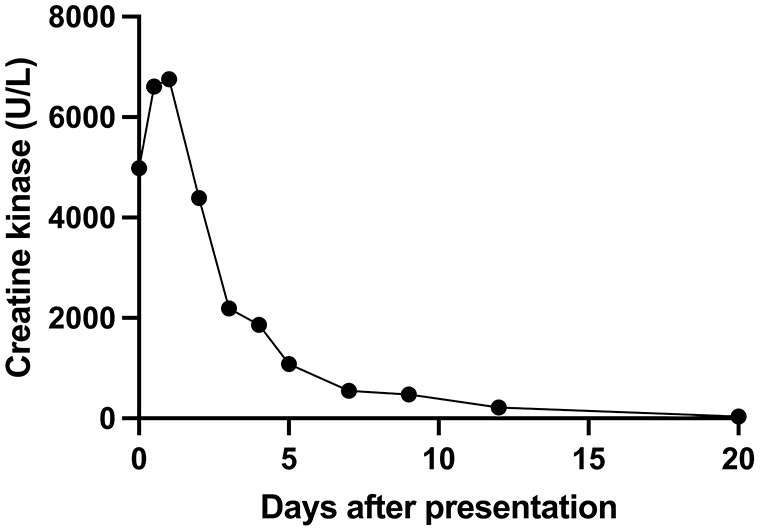
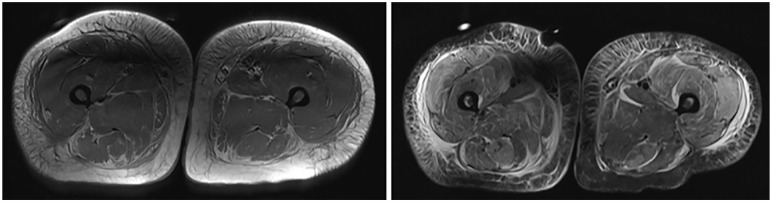
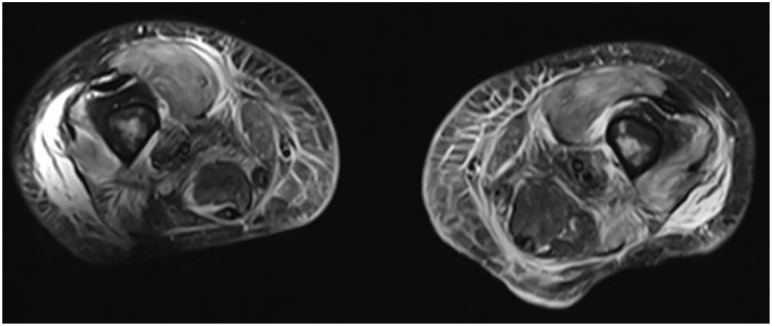
Human epidermal growth factor receptor-positive breast cancer is an aggressive cancer which represents approximately a quarter of all breast cancers worldwide. Recent advances have led to the development of targeted therapies, such as trastuzumab (H), which have significantly improved prognosis. Such therapies are currently used alongside other chemotherapeutic agents, such as paclitaxel (P) and gemcitabine (G). The most common side effects of PGH combination therapy include thrombocytopenia and anemias. However, there have been no previous reports of myositis resulting from this combination. We report the case of a 54-year-old metastatic breast cancer patient on PGH therapy who developed muscle weakness. The patient was initially treated with trastuzumab, pertuzumab, and paclitaxel. However, pertuzumab was changed to gemcitabine due to severe diarrhea. After the fourth cycle of PGH, the patient presented with muscle weakness and creatine kinase levels of up to 6755 U/L. Magnetic resonance imaging of the femur and pelvis revealed diffuse bilateral myositis, suggesting a diagnosis of gemcitabine-induced myositis. The patient was placed on intravenous fluids and corticosteroids, which resolved her condition. To our knowledge, this is the first report of gemcitabine-induced myositis in a breast cancer patient. Further studies are needed to determine the underlying mechanisms of gemcitabine-induced myositis and develop preventative measures.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


