Pramod Adiga, Sanjay Ramachandra Pudakalkatti, V Shivakumar, Mayank Jain, R Navaneeth Sreenidhi, C S Manohar, Sreenivas Jayaram, M Nagabhushan, Ramaiah Keshavamurthy
{"title":"慢性肾病患者经皮肾镜取石安全吗?","authors":"Pramod Adiga, Sanjay Ramachandra Pudakalkatti, V Shivakumar, Mayank Jain, R Navaneeth Sreenidhi, C S Manohar, Sreenivas Jayaram, M Nagabhushan, Ramaiah Keshavamurthy","doi":"10.4103/ua.ua_100_21","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Management of renal calculus in a patient of chronic kidney disease (CKD) is always challenging. Treatment options include extracorporeal shock wave lithotripsy, retrograde intrarenal surgery, and percutaneous nephrolithotomy (PCNL). With PCNL being gold standard for renal calculus ≥1.5 cm in normal kidneys, we aimed to analyze the safety and efficacy of PCNL in CKD patients with calculus ≥1.5 cm.</p><p><strong>Materials and methods: </strong>Sixty patients of CKD with renal calculus were included in the study: Group A with glomerular filtration rate (GFR) ≤30 ml/min/m<sup>2</sup> and Group B with GFR >30 <60 ml/min/m<sup>2</sup>. The estimated GFR (eGFR) pre-PCNL, peak eGFR on follow-up, and eGFR at last follow-up, stone free rates, and complications were recorded. The CKD stage before and after PCNL were also compared at the last follow-up.</p><p><strong>Results: </strong>The mean age of patients was 52 years. A mean of 1.14sittings per renal unit was required for PCNL. Complete clearance was 94% after all auxiliary procedures. The mean prePCNL eGFR was 26.5 ± 4.01 and 43.6 ± 9l. 14 ml/min/1.73 m<sup>2</sup> in Groups A and B, respectively. The mean post-PCNL eGFR was 32 ± 9.94 and 51 ± 8.85 ml/minute/1.73 m2, respectively, in Groups A and B. At a mean follow-up of 180 days, deterioration with the migration of CKD stage was seen in 13 patients (21.6%) out of which 10 patients were of Groups A and 3 in Group B. Six patients (10%) required maintenance hemodialysis. Postoperative bleeding complication requiring blood transfusions was seen in 12 (20%) and 3 (5%) required intensive care unit care postoperatively. No mortality was observed in our study.</p><p><strong>Conclusion: </strong>PCNL is an effective management strategy for renal calculus in patients with CKD with an acceptable stone clearance rates and manageable complications. Peak eGFR <30 ml/min/m2 and postprocedure complications predict deterioration and need for RRT.</p>","PeriodicalId":23633,"journal":{"name":"Urology Annals","volume":"14 4","pages":"317-321"},"PeriodicalIF":0.7000,"publicationDate":"2022-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/6d/b6/UA-14-317.PMC9731184.pdf","citationCount":"0","resultStr":"{\"title\":\"Is percutaneous nephrolithotomy safe in chronic kidney disease patients!!!\",\"authors\":\"Pramod Adiga, Sanjay Ramachandra Pudakalkatti, V Shivakumar, Mayank Jain, R Navaneeth Sreenidhi, C S Manohar, Sreenivas Jayaram, M Nagabhushan, Ramaiah Keshavamurthy\",\"doi\":\"10.4103/ua.ua_100_21\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Management of renal calculus in a patient of chronic kidney disease (CKD) is always challenging. Treatment options include extracorporeal shock wave lithotripsy, retrograde intrarenal surgery, and percutaneous nephrolithotomy (PCNL). With PCNL being gold standard for renal calculus ≥1.5 cm in normal kidneys, we aimed to analyze the safety and efficacy of PCNL in CKD patients with calculus ≥1.5 cm.</p><p><strong>Materials and methods: </strong>Sixty patients of CKD with renal calculus were included in the study: Group A with glomerular filtration rate (GFR) ≤30 ml/min/m<sup>2</sup> and Group B with GFR >30 <60 ml/min/m<sup>2</sup>. The estimated GFR (eGFR) pre-PCNL, peak eGFR on follow-up, and eGFR at last follow-up, stone free rates, and complications were recorded. The CKD stage before and after PCNL were also compared at the last follow-up.</p><p><strong>Results: </strong>The mean age of patients was 52 years. A mean of 1.14sittings per renal unit was required for PCNL. Complete clearance was 94% after all auxiliary procedures. The mean prePCNL eGFR was 26.5 ± 4.01 and 43.6 ± 9l. 14 ml/min/1.73 m<sup>2</sup> in Groups A and B, respectively. The mean post-PCNL eGFR was 32 ± 9.94 and 51 ± 8.85 ml/minute/1.73 m2, respectively, in Groups A and B. At a mean follow-up of 180 days, deterioration with the migration of CKD stage was seen in 13 patients (21.6%) out of which 10 patients were of Groups A and 3 in Group B. Six patients (10%) required maintenance hemodialysis. Postoperative bleeding complication requiring blood transfusions was seen in 12 (20%) and 3 (5%) required intensive care unit care postoperatively. No mortality was observed in our study.</p><p><strong>Conclusion: </strong>PCNL is an effective management strategy for renal calculus in patients with CKD with an acceptable stone clearance rates and manageable complications. Peak eGFR <30 ml/min/m2 and postprocedure complications predict deterioration and need for RRT.</p>\",\"PeriodicalId\":23633,\"journal\":{\"name\":\"Urology Annals\",\"volume\":\"14 4\",\"pages\":\"317-321\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2022-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/6d/b6/UA-14-317.PMC9731184.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Urology Annals\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/ua.ua_100_21\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Urology Annals","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/ua.ua_100_21","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
Is percutaneous nephrolithotomy safe in chronic kidney disease patients!!!
Introduction: Management of renal calculus in a patient of chronic kidney disease (CKD) is always challenging. Treatment options include extracorporeal shock wave lithotripsy, retrograde intrarenal surgery, and percutaneous nephrolithotomy (PCNL). With PCNL being gold standard for renal calculus ≥1.5 cm in normal kidneys, we aimed to analyze the safety and efficacy of PCNL in CKD patients with calculus ≥1.5 cm.
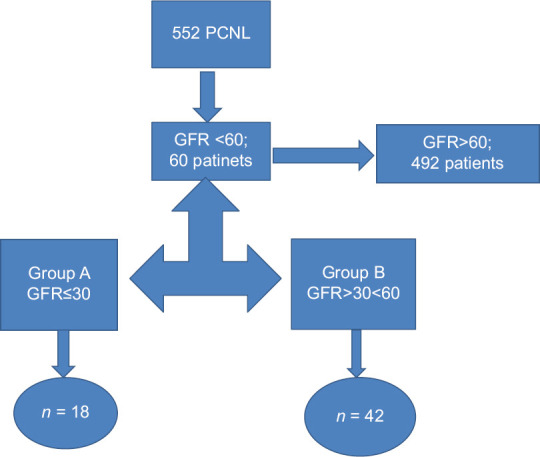
Materials and methods: Sixty patients of CKD with renal calculus were included in the study: Group A with glomerular filtration rate (GFR) ≤30 ml/min/m2 and Group B with GFR >30 <60 ml/min/m2. The estimated GFR (eGFR) pre-PCNL, peak eGFR on follow-up, and eGFR at last follow-up, stone free rates, and complications were recorded. The CKD stage before and after PCNL were also compared at the last follow-up.
Results: The mean age of patients was 52 years. A mean of 1.14sittings per renal unit was required for PCNL. Complete clearance was 94% after all auxiliary procedures. The mean prePCNL eGFR was 26.5 ± 4.01 and 43.6 ± 9l. 14 ml/min/1.73 m2 in Groups A and B, respectively. The mean post-PCNL eGFR was 32 ± 9.94 and 51 ± 8.85 ml/minute/1.73 m2, respectively, in Groups A and B. At a mean follow-up of 180 days, deterioration with the migration of CKD stage was seen in 13 patients (21.6%) out of which 10 patients were of Groups A and 3 in Group B. Six patients (10%) required maintenance hemodialysis. Postoperative bleeding complication requiring blood transfusions was seen in 12 (20%) and 3 (5%) required intensive care unit care postoperatively. No mortality was observed in our study.
Conclusion: PCNL is an effective management strategy for renal calculus in patients with CKD with an acceptable stone clearance rates and manageable complications. Peak eGFR <30 ml/min/m2 and postprocedure complications predict deterioration and need for RRT.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


