{"title":"机器学习算法作为单倍体造血干细胞移植后爱泼斯坦-巴尔病毒再激活的预测工具。","authors":"Shuang Fan, Hao-Yang Hong, Xin-Yu Dong, Lan-Ping Xu, Xiao-Hui Zhang, Yu Wang, Chen-Hua Yan, Huan Chen, Yu-Hong Chen, Wei Han, Feng-Rong Wang, Jing-Zhi Wang, Kai-Yan Liu, Meng-Zhu Shen, Xiao-Jun Huang, Shen-Da Hong, Xiao-Dong Mo","doi":"10.1097/BS9.0000000000000143","DOIUrl":null,"url":null,"abstract":"<p><p>Epstein-Barr virus (EBV) reactivation is one of the most important infections after hematopoietic stem cell transplantation (HSCT) using haplo-identical related donors (HID). We aimed to establish a comprehensive model with machine learning, which could predict EBV reactivation after HID HSCT with anti-thymocyte globulin (ATG) for graft-versus-host disease (GVHD) prophylaxis. We enrolled 470 consecutive acute leukemia patients, 60% of them (n = 282) randomly selected as a training cohort, the remaining 40% (n = 188) as a validation cohort. The equation was as follows: Probability (EBV reactivation) = <math><mstyle><mtext> </mtext> <mfrac><mn>1</mn> <mrow><mn>1</mn> <mrow><mtext> </mtext></mrow> <mtext> </mtext> <mrow><mtext> </mtext></mrow> <mo>+</mo> <mrow><mtext> </mtext></mrow> <mtext> </mtext> <mrow><mtext> </mtext> <mi>e</mi> <mi>x</mi> <mi>p</mi></mrow> <mrow><mo>(</mo> <mo>-</mo> <mrow><mi>Y</mi></mrow> <mo>)</mo></mrow> </mrow> </mfrac> </mstyle> </math> , where Y = 0.0250 × (age) - 0.3614 × (gender) + 0.0668 × (underlying disease) - 0.6297 × (disease status before HSCT) - 0.0726 × (disease risk index) - 0.0118 × (hematopoietic cell transplantation-specific comorbidity index [HCT-CI] score) + 1.2037 × (human leukocyte antigen disparity) + 0.5347 × (EBV serostatus) + 0.1605 × (conditioning regimen) - 0.2270 × (donor/recipient gender matched) + 0.2304 × (donor/recipient relation) - 0.0170 × (mononuclear cell counts in graft) + 0.0395 × (CD34+ cell count in graft) - 2.4510. The threshold of probability was 0.4623, which separated patients into low- and high-risk groups. The 1-year cumulative incidence of EBV reactivation in the low- and high-risk groups was 11.0% versus 24.5% (<i>P</i> < .001), 10.7% versus 19.3% (<i>P</i> = .046), and 11.4% versus 31.6% (<i>P</i> = .001), respectively, in total, training and validation cohorts. The model could also predict relapse and survival after HID HSCT. We established a comprehensive model that could predict EBV reactivation in HID HSCT recipients using ATG for GVHD prophylaxis.</p>","PeriodicalId":67343,"journal":{"name":"血液科学(英文)","volume":"5 1","pages":"51-59"},"PeriodicalIF":1.5000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9891443/pdf/","citationCount":"2","resultStr":"{\"title\":\"Machine learning algorithm as a prognostic tool for Epstein-Barr virus reactivation after haploidentical hematopoietic stem cell transplantation.\",\"authors\":\"Shuang Fan, Hao-Yang Hong, Xin-Yu Dong, Lan-Ping Xu, Xiao-Hui Zhang, Yu Wang, Chen-Hua Yan, Huan Chen, Yu-Hong Chen, Wei Han, Feng-Rong Wang, Jing-Zhi Wang, Kai-Yan Liu, Meng-Zhu Shen, Xiao-Jun Huang, Shen-Da Hong, Xiao-Dong Mo\",\"doi\":\"10.1097/BS9.0000000000000143\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Epstein-Barr virus (EBV) reactivation is one of the most important infections after hematopoietic stem cell transplantation (HSCT) using haplo-identical related donors (HID). We aimed to establish a comprehensive model with machine learning, which could predict EBV reactivation after HID HSCT with anti-thymocyte globulin (ATG) for graft-versus-host disease (GVHD) prophylaxis. We enrolled 470 consecutive acute leukemia patients, 60% of them (n = 282) randomly selected as a training cohort, the remaining 40% (n = 188) as a validation cohort. The equation was as follows: Probability (EBV reactivation) = <math><mstyle><mtext> </mtext> <mfrac><mn>1</mn> <mrow><mn>1</mn> <mrow><mtext> </mtext></mrow> <mtext> </mtext> <mrow><mtext> </mtext></mrow> <mo>+</mo> <mrow><mtext> </mtext></mrow> <mtext> </mtext> <mrow><mtext> </mtext> <mi>e</mi> <mi>x</mi> <mi>p</mi></mrow> <mrow><mo>(</mo> <mo>-</mo> <mrow><mi>Y</mi></mrow> <mo>)</mo></mrow> </mrow> </mfrac> </mstyle> </math> , where Y = 0.0250 × (age) - 0.3614 × (gender) + 0.0668 × (underlying disease) - 0.6297 × (disease status before HSCT) - 0.0726 × (disease risk index) - 0.0118 × (hematopoietic cell transplantation-specific comorbidity index [HCT-CI] score) + 1.2037 × (human leukocyte antigen disparity) + 0.5347 × (EBV serostatus) + 0.1605 × (conditioning regimen) - 0.2270 × (donor/recipient gender matched) + 0.2304 × (donor/recipient relation) - 0.0170 × (mononuclear cell counts in graft) + 0.0395 × (CD34+ cell count in graft) - 2.4510. The threshold of probability was 0.4623, which separated patients into low- and high-risk groups. The 1-year cumulative incidence of EBV reactivation in the low- and high-risk groups was 11.0% versus 24.5% (<i>P</i> < .001), 10.7% versus 19.3% (<i>P</i> = .046), and 11.4% versus 31.6% (<i>P</i> = .001), respectively, in total, training and validation cohorts. The model could also predict relapse and survival after HID HSCT. We established a comprehensive model that could predict EBV reactivation in HID HSCT recipients using ATG for GVHD prophylaxis.</p>\",\"PeriodicalId\":67343,\"journal\":{\"name\":\"血液科学(英文)\",\"volume\":\"5 1\",\"pages\":\"51-59\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9891443/pdf/\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"血液科学(英文)\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/BS9.0000000000000143\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"血液科学(英文)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/BS9.0000000000000143","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"HEMATOLOGY","Score":null,"Total":0}
Machine learning algorithm as a prognostic tool for Epstein-Barr virus reactivation after haploidentical hematopoietic stem cell transplantation.
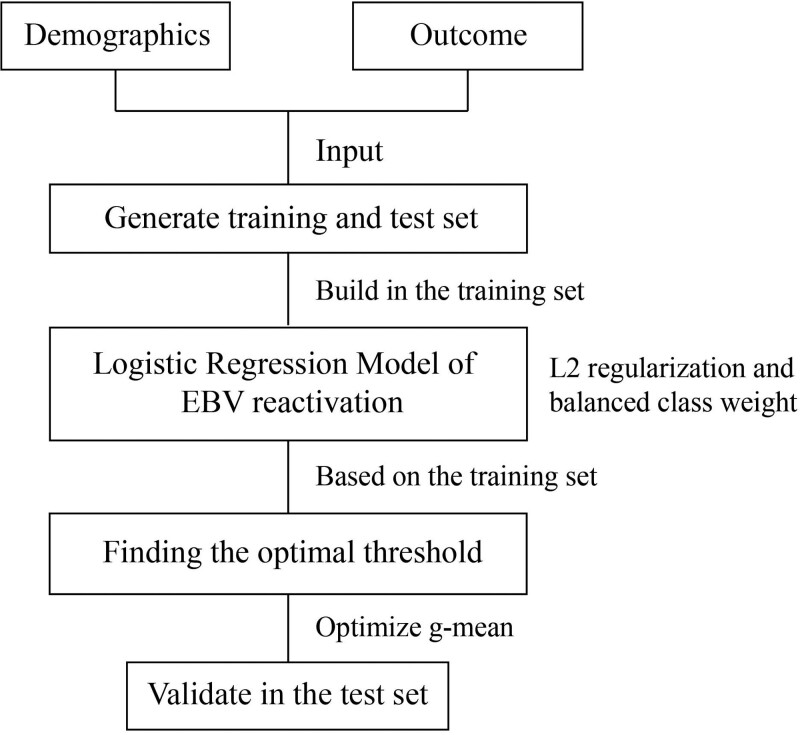
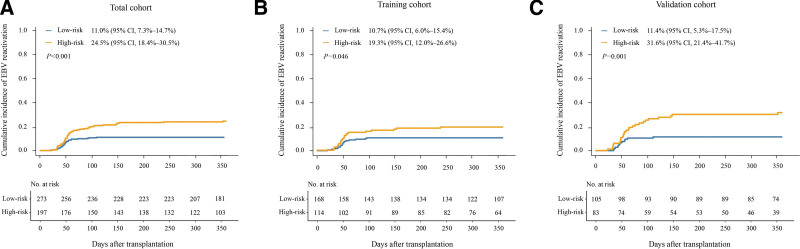
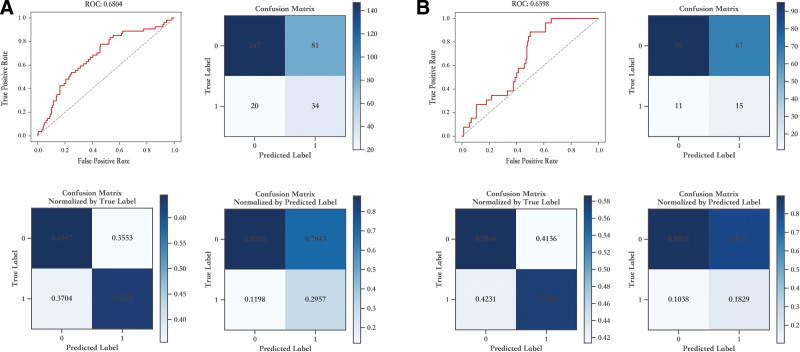
Epstein-Barr virus (EBV) reactivation is one of the most important infections after hematopoietic stem cell transplantation (HSCT) using haplo-identical related donors (HID). We aimed to establish a comprehensive model with machine learning, which could predict EBV reactivation after HID HSCT with anti-thymocyte globulin (ATG) for graft-versus-host disease (GVHD) prophylaxis. We enrolled 470 consecutive acute leukemia patients, 60% of them (n = 282) randomly selected as a training cohort, the remaining 40% (n = 188) as a validation cohort. The equation was as follows: Probability (EBV reactivation) = , where Y = 0.0250 × (age) - 0.3614 × (gender) + 0.0668 × (underlying disease) - 0.6297 × (disease status before HSCT) - 0.0726 × (disease risk index) - 0.0118 × (hematopoietic cell transplantation-specific comorbidity index [HCT-CI] score) + 1.2037 × (human leukocyte antigen disparity) + 0.5347 × (EBV serostatus) + 0.1605 × (conditioning regimen) - 0.2270 × (donor/recipient gender matched) + 0.2304 × (donor/recipient relation) - 0.0170 × (mononuclear cell counts in graft) + 0.0395 × (CD34+ cell count in graft) - 2.4510. The threshold of probability was 0.4623, which separated patients into low- and high-risk groups. The 1-year cumulative incidence of EBV reactivation in the low- and high-risk groups was 11.0% versus 24.5% (P < .001), 10.7% versus 19.3% (P = .046), and 11.4% versus 31.6% (P = .001), respectively, in total, training and validation cohorts. The model could also predict relapse and survival after HID HSCT. We established a comprehensive model that could predict EBV reactivation in HID HSCT recipients using ATG for GVHD prophylaxis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


