{"title":"保留射血分数和房颤打破心力衰竭的循环。","authors":"Otilia Ţica, Waseem Khamboo, Dipak Kotecha","doi":"10.15420/cfr.2022.03","DOIUrl":null,"url":null,"abstract":"<p><p>Heart failure with preserved ejection fraction (HFpEF) and AF are two common cardiovascular conditions that are inextricably linked to each other's development and progression, often in multimorbid patients. Current management is often directed to specific components of each disease without considering their joint impact on diagnosis, treatment and prognosis. The result for patients is suboptimal on all three levels, restricting clinicians from preventing major adverse events, including death, which occurs in 20% of patients at 2 years and in 45% at 4 years. New trial evidence and reanalysis of prior trials are providing a glimmer of hope that adverse outcomes can be reduced in those with concurrent HFpEF and AF. This will require a restructuring of care to integrate heart failure and AF teams, alongside those that manage comorbidities. Parallel commencement and non-sequential uptitration of therapeutics across different domains will be vital to ensure that all patients benefit at a personal level, based on their own needs and priorities.</p>","PeriodicalId":33741,"journal":{"name":"Cardiac Failure Review","volume":"8 ","pages":"e32"},"PeriodicalIF":5.7000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a4/65/cfr-08-e32.PMC9820207.pdf","citationCount":"2","resultStr":"{\"title\":\"Breaking the Cycle of Heart Failure With Preserved Ejection Fraction and Atrial Fibrillation.\",\"authors\":\"Otilia Ţica, Waseem Khamboo, Dipak Kotecha\",\"doi\":\"10.15420/cfr.2022.03\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Heart failure with preserved ejection fraction (HFpEF) and AF are two common cardiovascular conditions that are inextricably linked to each other's development and progression, often in multimorbid patients. Current management is often directed to specific components of each disease without considering their joint impact on diagnosis, treatment and prognosis. The result for patients is suboptimal on all three levels, restricting clinicians from preventing major adverse events, including death, which occurs in 20% of patients at 2 years and in 45% at 4 years. New trial evidence and reanalysis of prior trials are providing a glimmer of hope that adverse outcomes can be reduced in those with concurrent HFpEF and AF. This will require a restructuring of care to integrate heart failure and AF teams, alongside those that manage comorbidities. Parallel commencement and non-sequential uptitration of therapeutics across different domains will be vital to ensure that all patients benefit at a personal level, based on their own needs and priorities.</p>\",\"PeriodicalId\":33741,\"journal\":{\"name\":\"Cardiac Failure Review\",\"volume\":\"8 \",\"pages\":\"e32\"},\"PeriodicalIF\":5.7000,\"publicationDate\":\"2022-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a4/65/cfr-08-e32.PMC9820207.pdf\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cardiac Failure Review\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.15420/cfr.2022.03\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiac Failure Review","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.15420/cfr.2022.03","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Breaking the Cycle of Heart Failure With Preserved Ejection Fraction and Atrial Fibrillation.
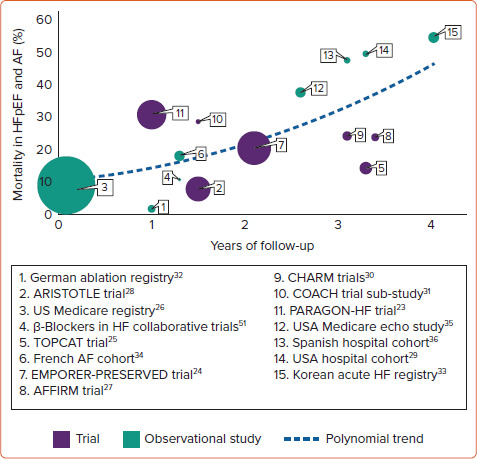
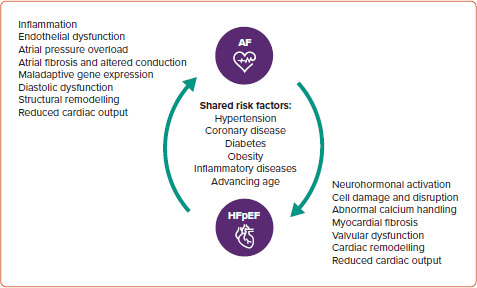
Heart failure with preserved ejection fraction (HFpEF) and AF are two common cardiovascular conditions that are inextricably linked to each other's development and progression, often in multimorbid patients. Current management is often directed to specific components of each disease without considering their joint impact on diagnosis, treatment and prognosis. The result for patients is suboptimal on all three levels, restricting clinicians from preventing major adverse events, including death, which occurs in 20% of patients at 2 years and in 45% at 4 years. New trial evidence and reanalysis of prior trials are providing a glimmer of hope that adverse outcomes can be reduced in those with concurrent HFpEF and AF. This will require a restructuring of care to integrate heart failure and AF teams, alongside those that manage comorbidities. Parallel commencement and non-sequential uptitration of therapeutics across different domains will be vital to ensure that all patients benefit at a personal level, based on their own needs and priorities.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


