{"title":"造血干细胞移植受者急性胰腺炎的住院疗效。","authors":"Hunza Chaudhry, Armaan Dhaliwal, Kanwal Bains, Aalam Sohal, Piyush Singla, Raghav Sharma, Dino Dukovic, Isha Kohli, Gagan Gupta, Devang Prajapati","doi":"10.14740/gr1579","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Acute pancreatitis (AP) carries a significant morbidity and mortality worldwide. AP is a potential complication of hematopoietic stem cell transplantation (HSCT) although its incidence remains unclear. HSCT recipients are at increased risk of AP due to various factors but the effect of AP on mortality and resource utilization in the adult population has not been studied. We investigated the impact of AP on hospitalization outcomes among patients following HSCT.</p><p><strong>Methods: </strong>We queried the National Inpatient Sample (NIS) database using the International Classification of Diseases (ICD)-10 codes. All adult patients with a diagnosis or procedure code of HSCT were included in the study. Patients were divided into those with a diagnosis of AP and those without. Sensitivity analysis was performed for patients with a length of stay greater than 28 days. The relationship between AP and mortality, length of stay, total hospitalization cost, and charges was assessed using univariate analysis followed by multivariate analysis.</p><p><strong>Results: </strong>Of the 140,130 adult patients with HSCT, 855 (0.61%) patients developed AP. There was 1.74 times higher risk of mortality in patients with AP as compared to controls (adjusted odds ratio (aOR): 1.74, P = 0.0055). There was no statistically significant difference in the length of stay, hospitalization charge, or cost before sensitivity analysis. After sensitivity analysis, 13,240 patients were included, from which 125 (0.94%) had AP. There was 3.85 times higher risk of mortality in patients who developed AP as compared to controls (aOR: 3.85, P = 0.003). There was a statistically significant increase noted in the length of stay (adj coeff: 20.3 days, P = 0.002), hospital charges (+$346,616, P = 0.017), and cost (+$121,932.4, P = 0.001) in patients with AP as compared to those who did not develop AP.</p><p><strong>Conclusion: </strong>Recipients of HSCT who develop AP have shown to have higher mortality on sensitivity analysis. This study highlights that AP in HSCT patients is associated with worse outcomes and higher resource utilization. Physicians should be aware of this association as the presence of pancreatitis portends a poor prognosis.</p>","PeriodicalId":12461,"journal":{"name":"Gastroenterology Research","volume":"15 6","pages":"334-342"},"PeriodicalIF":1.7000,"publicationDate":"2022-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/53/44/gr-15-334.PMC9822663.pdf","citationCount":"2","resultStr":"{\"title\":\"Hospitalization Outcomes of Acute Pancreatitis in Hematopoietic Stem Cell Transplant Recipients.\",\"authors\":\"Hunza Chaudhry, Armaan Dhaliwal, Kanwal Bains, Aalam Sohal, Piyush Singla, Raghav Sharma, Dino Dukovic, Isha Kohli, Gagan Gupta, Devang Prajapati\",\"doi\":\"10.14740/gr1579\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Acute pancreatitis (AP) carries a significant morbidity and mortality worldwide. AP is a potential complication of hematopoietic stem cell transplantation (HSCT) although its incidence remains unclear. HSCT recipients are at increased risk of AP due to various factors but the effect of AP on mortality and resource utilization in the adult population has not been studied. We investigated the impact of AP on hospitalization outcomes among patients following HSCT.</p><p><strong>Methods: </strong>We queried the National Inpatient Sample (NIS) database using the International Classification of Diseases (ICD)-10 codes. All adult patients with a diagnosis or procedure code of HSCT were included in the study. Patients were divided into those with a diagnosis of AP and those without. Sensitivity analysis was performed for patients with a length of stay greater than 28 days. The relationship between AP and mortality, length of stay, total hospitalization cost, and charges was assessed using univariate analysis followed by multivariate analysis.</p><p><strong>Results: </strong>Of the 140,130 adult patients with HSCT, 855 (0.61%) patients developed AP. There was 1.74 times higher risk of mortality in patients with AP as compared to controls (adjusted odds ratio (aOR): 1.74, P = 0.0055). There was no statistically significant difference in the length of stay, hospitalization charge, or cost before sensitivity analysis. After sensitivity analysis, 13,240 patients were included, from which 125 (0.94%) had AP. There was 3.85 times higher risk of mortality in patients who developed AP as compared to controls (aOR: 3.85, P = 0.003). There was a statistically significant increase noted in the length of stay (adj coeff: 20.3 days, P = 0.002), hospital charges (+$346,616, P = 0.017), and cost (+$121,932.4, P = 0.001) in patients with AP as compared to those who did not develop AP.</p><p><strong>Conclusion: </strong>Recipients of HSCT who develop AP have shown to have higher mortality on sensitivity analysis. This study highlights that AP in HSCT patients is associated with worse outcomes and higher resource utilization. Physicians should be aware of this association as the presence of pancreatitis portends a poor prognosis.</p>\",\"PeriodicalId\":12461,\"journal\":{\"name\":\"Gastroenterology Research\",\"volume\":\"15 6\",\"pages\":\"334-342\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2022-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/53/44/gr-15-334.PMC9822663.pdf\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Gastroenterology Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14740/gr1579\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Gastroenterology Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/gr1579","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 2
摘要
背景:急性胰腺炎(AP)在世界范围内具有显著的发病率和死亡率。AP是造血干细胞移植(HSCT)的潜在并发症,尽管其发病率尚不清楚。由于各种因素,HSCT受者AP的风险增加,但AP对成人死亡率和资源利用的影响尚未研究。我们调查了AP对HSCT患者住院结果的影响。方法:使用国际疾病分类(ICD)-10代码查询国家住院患者样本(NIS)数据库。所有诊断为HSCT或手术代码为HSCT的成年患者均被纳入研究。患者分为诊断为AP的患者和未诊断为AP的患者。对住院时间大于28天的患者进行敏感性分析。采用单因素分析和多因素分析评估AP与死亡率、住院时间、总住院费用和收费之间的关系。结果:在140130例成人HSCT患者中,855例(0.61%)患者发生AP。AP患者的死亡率是对照组的1.74倍(调整后的优势比(aOR): 1.74, P = 0.0055)。敏感性分析前,两组患者的住院时间、住院费用、费用差异无统计学意义。敏感性分析后,纳入13240例患者,其中125例(0.94%)患有AP。与对照组相比,发生AP的患者死亡风险高3.85倍(aOR: 3.85, P = 0.003)。与未发生AP的患者相比,AP患者的住院时间(20.3天,P = 0.002)、住院费用(+ 346,616美元,P = 0.017)和费用(+ 121,932.4美元,P = 0.001)均有统计学意义上的显著增加。结论:敏感性分析显示,发生AP的HSCT患者死亡率更高。本研究强调,HSCT患者的AP与较差的预后和较高的资源利用率相关。医生应该意识到这种关联,因为胰腺炎的存在预示着预后不良。
Hospitalization Outcomes of Acute Pancreatitis in Hematopoietic Stem Cell Transplant Recipients.
Background: Acute pancreatitis (AP) carries a significant morbidity and mortality worldwide. AP is a potential complication of hematopoietic stem cell transplantation (HSCT) although its incidence remains unclear. HSCT recipients are at increased risk of AP due to various factors but the effect of AP on mortality and resource utilization in the adult population has not been studied. We investigated the impact of AP on hospitalization outcomes among patients following HSCT.
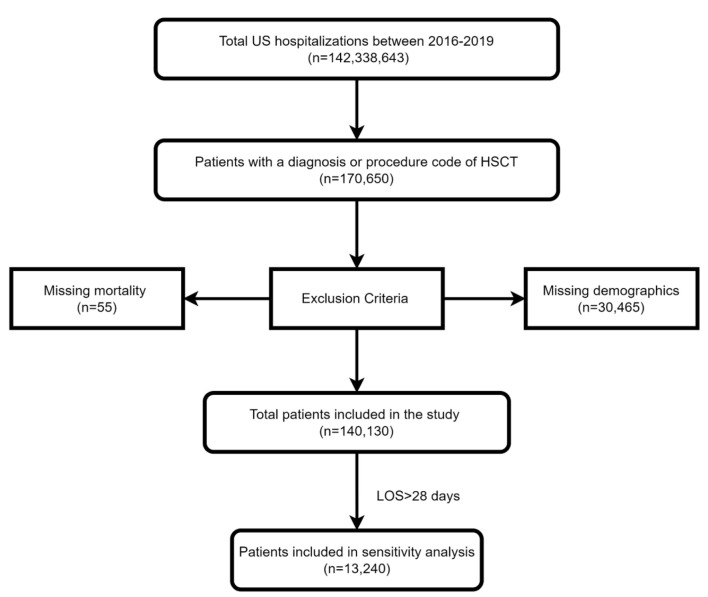
Methods: We queried the National Inpatient Sample (NIS) database using the International Classification of Diseases (ICD)-10 codes. All adult patients with a diagnosis or procedure code of HSCT were included in the study. Patients were divided into those with a diagnosis of AP and those without. Sensitivity analysis was performed for patients with a length of stay greater than 28 days. The relationship between AP and mortality, length of stay, total hospitalization cost, and charges was assessed using univariate analysis followed by multivariate analysis.
Results: Of the 140,130 adult patients with HSCT, 855 (0.61%) patients developed AP. There was 1.74 times higher risk of mortality in patients with AP as compared to controls (adjusted odds ratio (aOR): 1.74, P = 0.0055). There was no statistically significant difference in the length of stay, hospitalization charge, or cost before sensitivity analysis. After sensitivity analysis, 13,240 patients were included, from which 125 (0.94%) had AP. There was 3.85 times higher risk of mortality in patients who developed AP as compared to controls (aOR: 3.85, P = 0.003). There was a statistically significant increase noted in the length of stay (adj coeff: 20.3 days, P = 0.002), hospital charges (+$346,616, P = 0.017), and cost (+$121,932.4, P = 0.001) in patients with AP as compared to those who did not develop AP.
Conclusion: Recipients of HSCT who develop AP have shown to have higher mortality on sensitivity analysis. This study highlights that AP in HSCT patients is associated with worse outcomes and higher resource utilization. Physicians should be aware of this association as the presence of pancreatitis portends a poor prognosis.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


