Zhong Wang, Ruijian Zhang, Zhitong Han, Yisong Zhang, Junqing Wang, Bo Wang, Baiyu Liu, Weiran Yang
{"title":"颅内峰值压作为自发性脑出血引流和减压颅骨切除术后围手术期死亡率的预测因子。","authors":"Zhong Wang, Ruijian Zhang, Zhitong Han, Yisong Zhang, Junqing Wang, Bo Wang, Baiyu Liu, Weiran Yang","doi":"10.1186/s41016-023-00316-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>An optimal intracranial pressure (ICP) management target is not well defined in patients with spontaneous intracerebral hemorrhage. The aim of this study was to explore the association between perioperative ICP monitoring parameters and mortality of patients with spontaneous intracerebral hematoma undergoing emergency hematoma removal and decompressive craniectomy (DC), to provide evidence for a target-oriented ICP management.</p><p><strong>Methods: </strong>The clinical and radiological features of 176 consecutive patients with spontaneous intracerebral hemorrhage that underwent emergent hematoma evacuation and DC were reviewed. The Glasgow Coma Scale (GCS) and Glasgow Outcome Scale (GOS) scores were assessed 2 weeks after surgery. Multivariate logistic regression analysis was performed to identify predictors for perioperative death.</p><p><strong>Results: </strong>Forty-four cases (25.0%) were assigned to the ICP group. In patients with an ICP monitor, the median peak ICP value was 25.5 mmHg; 50% of them had a peak ICP value of more than 25 mmHg. The median duration of ICP > 25 mmHg was 2 days. Without a target-specific ICP management, the mortality at 2 weeks after surgery was similar between patients with or without an ICP monitor (27.3% versus 18.2%, p = 0.20). In multivariable analysis, the peak ICP value (OR 1.11, 95% CI 1.004-1.234, p = 0.04) was significantly associated with perioperative death in the ICP group. The area under ROC curve of peak ICP value was 0.78 (95%CI 0.62-0.94) for predicting mortality, with a cut-off value of 31 mmHg.</p><p><strong>Conclusion: </strong>Compared with a persistent hyperintracranial pressure, a high ICP peak value might provide a better prediction for the mortality of patients with spontaneous intracerebral hemorrhage evacuation and DC, suggesting a tailored ICP management protocol to decrease ICP peak value.</p>","PeriodicalId":36700,"journal":{"name":"Chinese Neurosurgical Journal","volume":"9 1","pages":"2"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9847089/pdf/","citationCount":"0","resultStr":"{\"title\":\"Intracranial peak pressure as a predictor for perioperative mortality after spontaneous intracerebral hemorrhage evacuation and decompressive craniectomy.\",\"authors\":\"Zhong Wang, Ruijian Zhang, Zhitong Han, Yisong Zhang, Junqing Wang, Bo Wang, Baiyu Liu, Weiran Yang\",\"doi\":\"10.1186/s41016-023-00316-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>An optimal intracranial pressure (ICP) management target is not well defined in patients with spontaneous intracerebral hemorrhage. The aim of this study was to explore the association between perioperative ICP monitoring parameters and mortality of patients with spontaneous intracerebral hematoma undergoing emergency hematoma removal and decompressive craniectomy (DC), to provide evidence for a target-oriented ICP management.</p><p><strong>Methods: </strong>The clinical and radiological features of 176 consecutive patients with spontaneous intracerebral hemorrhage that underwent emergent hematoma evacuation and DC were reviewed. The Glasgow Coma Scale (GCS) and Glasgow Outcome Scale (GOS) scores were assessed 2 weeks after surgery. Multivariate logistic regression analysis was performed to identify predictors for perioperative death.</p><p><strong>Results: </strong>Forty-four cases (25.0%) were assigned to the ICP group. In patients with an ICP monitor, the median peak ICP value was 25.5 mmHg; 50% of them had a peak ICP value of more than 25 mmHg. The median duration of ICP > 25 mmHg was 2 days. Without a target-specific ICP management, the mortality at 2 weeks after surgery was similar between patients with or without an ICP monitor (27.3% versus 18.2%, p = 0.20). In multivariable analysis, the peak ICP value (OR 1.11, 95% CI 1.004-1.234, p = 0.04) was significantly associated with perioperative death in the ICP group. The area under ROC curve of peak ICP value was 0.78 (95%CI 0.62-0.94) for predicting mortality, with a cut-off value of 31 mmHg.</p><p><strong>Conclusion: </strong>Compared with a persistent hyperintracranial pressure, a high ICP peak value might provide a better prediction for the mortality of patients with spontaneous intracerebral hemorrhage evacuation and DC, suggesting a tailored ICP management protocol to decrease ICP peak value.</p>\",\"PeriodicalId\":36700,\"journal\":{\"name\":\"Chinese Neurosurgical Journal\",\"volume\":\"9 1\",\"pages\":\"2\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-01-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9847089/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Chinese Neurosurgical Journal\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s41016-023-00316-5\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Chinese Neurosurgical Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s41016-023-00316-5","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
摘要
背景:自发性脑出血患者的最佳颅内压(ICP)管理目标尚未明确。本研究的目的是探讨自发性脑内血肿患者急诊血肿清除和减压颅脑切除术(DC)围手术期ICP监测参数与死亡率之间的关系,为有针对性的ICP治疗提供依据。方法:回顾性分析176例自发性脑出血患者的临床及影像学表现。术后2周评估格拉斯哥昏迷评分(GCS)和格拉斯哥结局评分(GOS)。进行多因素logistic回归分析以确定围手术期死亡的预测因素。结果:44例(25.0%)分为ICP组。在使用ICP监测仪的患者中,ICP峰值中位数为25.5 mmHg;其中50%的患者ICP峰值大于25mmhg。ICP > 25 mmHg的中位持续时间为2天。没有针对特定目标的ICP管理,术后2周死亡率在有或没有ICP监护的患者之间相似(27.3%对18.2%,p = 0.20)。在多变量分析中,ICP组的峰值ICP值(OR 1.11, 95% CI 1.004-1.234, p = 0.04)与围手术期死亡显著相关。预测死亡率的ROC曲线下面积为0.78 (95%CI 0.62 ~ 0.94),临界值为31 mmHg。结论:与持续高颅内压相比,高ICP峰值可更好地预测自发性脑出血引流和DC患者的死亡率,建议制定针对性的ICP管理方案,降低ICP峰值。
Intracranial peak pressure as a predictor for perioperative mortality after spontaneous intracerebral hemorrhage evacuation and decompressive craniectomy.
Background: An optimal intracranial pressure (ICP) management target is not well defined in patients with spontaneous intracerebral hemorrhage. The aim of this study was to explore the association between perioperative ICP monitoring parameters and mortality of patients with spontaneous intracerebral hematoma undergoing emergency hematoma removal and decompressive craniectomy (DC), to provide evidence for a target-oriented ICP management.
Methods: The clinical and radiological features of 176 consecutive patients with spontaneous intracerebral hemorrhage that underwent emergent hematoma evacuation and DC were reviewed. The Glasgow Coma Scale (GCS) and Glasgow Outcome Scale (GOS) scores were assessed 2 weeks after surgery. Multivariate logistic regression analysis was performed to identify predictors for perioperative death.
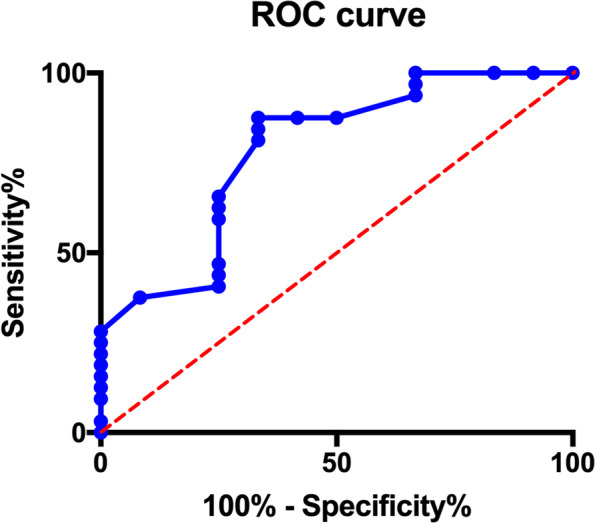
Results: Forty-four cases (25.0%) were assigned to the ICP group. In patients with an ICP monitor, the median peak ICP value was 25.5 mmHg; 50% of them had a peak ICP value of more than 25 mmHg. The median duration of ICP > 25 mmHg was 2 days. Without a target-specific ICP management, the mortality at 2 weeks after surgery was similar between patients with or without an ICP monitor (27.3% versus 18.2%, p = 0.20). In multivariable analysis, the peak ICP value (OR 1.11, 95% CI 1.004-1.234, p = 0.04) was significantly associated with perioperative death in the ICP group. The area under ROC curve of peak ICP value was 0.78 (95%CI 0.62-0.94) for predicting mortality, with a cut-off value of 31 mmHg.
Conclusion: Compared with a persistent hyperintracranial pressure, a high ICP peak value might provide a better prediction for the mortality of patients with spontaneous intracerebral hemorrhage evacuation and DC, suggesting a tailored ICP management protocol to decrease ICP peak value.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


