Damian M Bailey, George A Rose, Daniel O'Donovan, Dafydd Locker, Ian R Appadurai, Richard G Davies, Richard J Whiston, Mohamad Bashir, Michael H Lewis, Ian M Williams
{"title":"与经腹膜入路相比,经腹膜后入路治疗腹主动脉瘤可减少全身炎症和术后发病率。","authors":"Damian M Bailey, George A Rose, Daniel O'Donovan, Dafydd Locker, Ian R Appadurai, Richard G Davies, Richard J Whiston, Mohamad Bashir, Michael H Lewis, Ian M Williams","doi":"10.1055/s-0042-1749173","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong> In the United Kingdom, the most common surgical approach for repair of open abdominal aortic aneurysms (AAAs) is transperitoneal (TP). However, retroperitoneal (RP) approach is favored in those with more complex vascular anatomy often requiring a cross-clamp on the aorta superior to the renal arteries. This study compared these approaches in patients matched on all major demographic, comorbid, anatomic, and physiological variables.</p><p><strong>Methods: </strong> Fifty-seven patients (TP: <i>n</i> = 24; RP: <i>n</i> = 33) unsuitable for endovascular aneurysm repair underwent preoperative cardiopulmonary exercise testing prior to open AAA repair. The surgical approach undertaken was dictated by individual surgeon preference. Postoperative mortality, complications, and length of hospital stay (LoS) were recorded. Patients were further stratified according to infrarenal (IR) or suprarenal/supraceliac (SR/SC) surgical clamping. Systemic inflammation (C-reactive protein) and renal function (serum creatinine and estimated glomerular filtration rate) were recorded.</p><p><strong>Results: </strong> Twenty-three (96%) of TP patients only required an IR clamp compared with 12 (36%) in the RP group. Postoperative systemic inflammation was lower in RP patients (<i>p</i> = 0.002 vs. TP) and fewer reported pulmonary/gastrointestinal complications whereas renal impairment was more marked in those receiving SR/SC clamps (<i>p</i> < 0.001 vs. IR clamp). RP patients were defined by lower LoS (<i>p</i> = 0.001), while mid-/long-term mortality was low/comparable with TP, resulting in considerable cost savings.</p><p><strong>Conclusion: </strong> Despite the demands of more complicated vascular anatomy, the clinical and economic benefits highlighted by these findings justify the more routine adoption of the RP approach for complex AAA repair.</p>","PeriodicalId":52392,"journal":{"name":"AORTA","volume":null,"pages":null},"PeriodicalIF":0.0000,"publicationDate":"2022-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9767756/pdf/","citationCount":"2","resultStr":"{\"title\":\"Retroperitoneal Compared to Transperitoneal Approach for Open Abdominal Aortic Aneurysm Repair Is Associated with Reduced Systemic Inflammation and Postoperative Morbidity.\",\"authors\":\"Damian M Bailey, George A Rose, Daniel O'Donovan, Dafydd Locker, Ian R Appadurai, Richard G Davies, Richard J Whiston, Mohamad Bashir, Michael H Lewis, Ian M Williams\",\"doi\":\"10.1055/s-0042-1749173\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong> In the United Kingdom, the most common surgical approach for repair of open abdominal aortic aneurysms (AAAs) is transperitoneal (TP). However, retroperitoneal (RP) approach is favored in those with more complex vascular anatomy often requiring a cross-clamp on the aorta superior to the renal arteries. This study compared these approaches in patients matched on all major demographic, comorbid, anatomic, and physiological variables.</p><p><strong>Methods: </strong> Fifty-seven patients (TP: <i>n</i> = 24; RP: <i>n</i> = 33) unsuitable for endovascular aneurysm repair underwent preoperative cardiopulmonary exercise testing prior to open AAA repair. The surgical approach undertaken was dictated by individual surgeon preference. Postoperative mortality, complications, and length of hospital stay (LoS) were recorded. Patients were further stratified according to infrarenal (IR) or suprarenal/supraceliac (SR/SC) surgical clamping. Systemic inflammation (C-reactive protein) and renal function (serum creatinine and estimated glomerular filtration rate) were recorded.</p><p><strong>Results: </strong> Twenty-three (96%) of TP patients only required an IR clamp compared with 12 (36%) in the RP group. Postoperative systemic inflammation was lower in RP patients (<i>p</i> = 0.002 vs. TP) and fewer reported pulmonary/gastrointestinal complications whereas renal impairment was more marked in those receiving SR/SC clamps (<i>p</i> < 0.001 vs. IR clamp). RP patients were defined by lower LoS (<i>p</i> = 0.001), while mid-/long-term mortality was low/comparable with TP, resulting in considerable cost savings.</p><p><strong>Conclusion: </strong> Despite the demands of more complicated vascular anatomy, the clinical and economic benefits highlighted by these findings justify the more routine adoption of the RP approach for complex AAA repair.</p>\",\"PeriodicalId\":52392,\"journal\":{\"name\":\"AORTA\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9767756/pdf/\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"AORTA\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1055/s-0042-1749173\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"AORTA","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0042-1749173","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 2
摘要
背景:在英国,腹主动脉瘤(AAAs)最常见的手术方法是经腹膜(TP)。然而,腹膜后(RP)入路在血管解剖更复杂的患者中更受青睐,通常需要在肾动脉上方的主动脉上交叉夹紧。本研究比较了这些方法在所有主要人口统计学、合并症、解剖和生理变量匹配的患者中的应用。方法:57例患者(TP: n = 24;RP: n = 33)不适合血管内动脉瘤修复的患者在行AAA开腹修复前行术前心肺运动试验。所采取的手术入路是由个别外科医生的偏好决定的。记录术后死亡率、并发症和住院时间(LoS)。患者进一步分层根据肾下(IR)或肾上/腹腔上(SR/SC)手术夹紧。记录全身炎症(c反应蛋白)和肾功能(血清肌酐和肾小球滤过率)。结果:23例(96%)TP患者只需要IR钳,而RP组为12例(36%)。RP患者术后全身炎症较低(p = 0.002 vs. TP),报告的肺部/胃肠道并发症较少,而接受SR/SC钳的患者肾脏损害更为明显(p = 0.001),而中期/长期死亡率较低/与TP相当,从而节省了相当大的成本。结论:尽管需要更复杂的血管解剖,这些发现强调的临床和经济效益证明更常规地采用RP入路修复复杂的AAA。
Retroperitoneal Compared to Transperitoneal Approach for Open Abdominal Aortic Aneurysm Repair Is Associated with Reduced Systemic Inflammation and Postoperative Morbidity.
Background: In the United Kingdom, the most common surgical approach for repair of open abdominal aortic aneurysms (AAAs) is transperitoneal (TP). However, retroperitoneal (RP) approach is favored in those with more complex vascular anatomy often requiring a cross-clamp on the aorta superior to the renal arteries. This study compared these approaches in patients matched on all major demographic, comorbid, anatomic, and physiological variables.
Methods: Fifty-seven patients (TP: n = 24; RP: n = 33) unsuitable for endovascular aneurysm repair underwent preoperative cardiopulmonary exercise testing prior to open AAA repair. The surgical approach undertaken was dictated by individual surgeon preference. Postoperative mortality, complications, and length of hospital stay (LoS) were recorded. Patients were further stratified according to infrarenal (IR) or suprarenal/supraceliac (SR/SC) surgical clamping. Systemic inflammation (C-reactive protein) and renal function (serum creatinine and estimated glomerular filtration rate) were recorded.
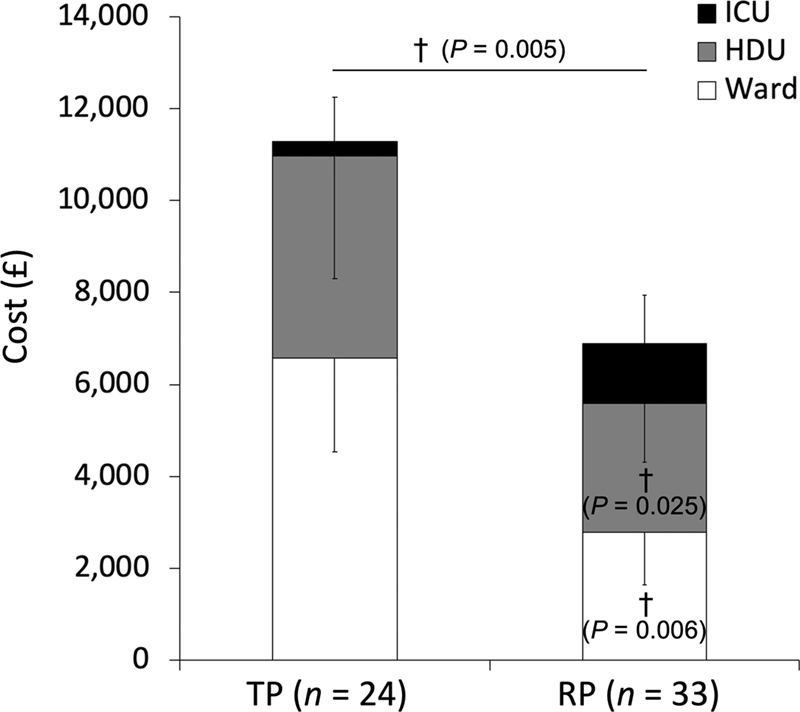
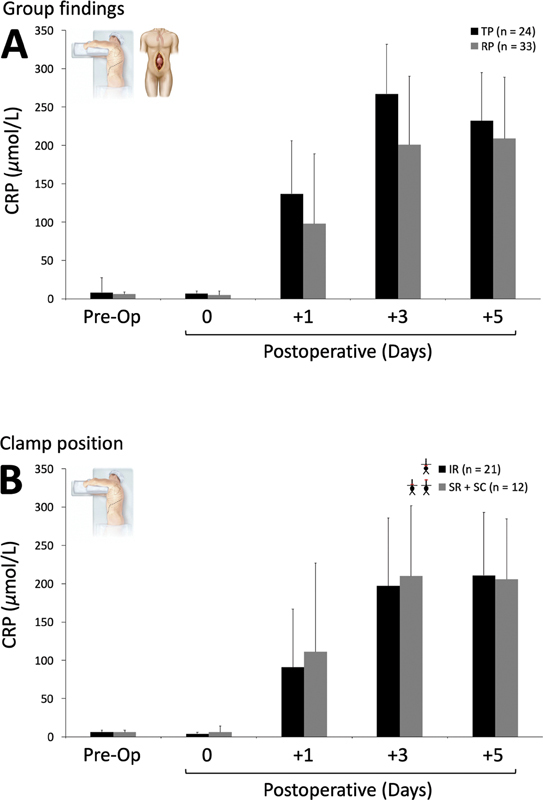
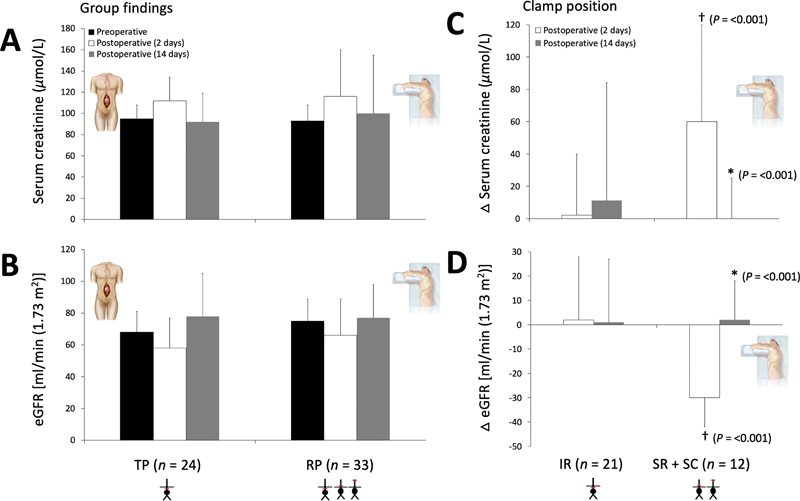
Results: Twenty-three (96%) of TP patients only required an IR clamp compared with 12 (36%) in the RP group. Postoperative systemic inflammation was lower in RP patients (p = 0.002 vs. TP) and fewer reported pulmonary/gastrointestinal complications whereas renal impairment was more marked in those receiving SR/SC clamps (p < 0.001 vs. IR clamp). RP patients were defined by lower LoS (p = 0.001), while mid-/long-term mortality was low/comparable with TP, resulting in considerable cost savings.
Conclusion: Despite the demands of more complicated vascular anatomy, the clinical and economic benefits highlighted by these findings justify the more routine adoption of the RP approach for complex AAA repair.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


