Guus C G H Blok, Eelke D Nikkels, Johan van der Lei, Marjolein Y Berger, Gea A Holtman
{"title":"在评估儿童阑尾炎时,CRP 对临床特征的附加值。","authors":"Guus C G H Blok, Eelke D Nikkels, Johan van der Lei, Marjolein Y Berger, Gea A Holtman","doi":"10.1080/13814788.2022.2067142","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The diagnostic value of C-reactive protein (CRP) for appendicitis in children has not been evaluated in primary care. As biochemical responses and differential diagnoses vary with age, separate evaluation in children and adults is needed.</p><p><strong>Objectives: </strong>To determine whether adding CRP to symptoms and signs improves the diagnosis of appendicitis in children with acute abdominal pain in primary care.</p><p><strong>Methods: </strong>A retrospective cohort study in Dutch general practice. Data was collected from the Integrated Primary Care Information database between 2010 and 2016. We included children aged 4-18 years, with no history of appendicitis, presenting with acute abdominal pain, and having a CRP test. Initial CRP levels were related to the specialist's diagnosis of appendicitis, and the test's characteristics were calculated for multiple cut-offs. The value of adding CRP to signs and symptoms was analysed by logistic regression.</p><p><strong>Results: </strong>We identified 1076 eligible children, among whom 203 were referred for specialist evaluation and 70 had appendicitis. The sensitivity and specificity of a CRP cut-off ≥10 mg/L were 0.87 (95%CI, 0.77-0.94) and 0.77 (95%CI, 0.74-0.79), respectively. When symptoms lasted > 48 h, this sensitivity increased to 1.00. Positive predictive values for CRP alone were low (0.18-0.38) for all cut-off values (6-100 mg/L). Adding CRP increased the area under the curve from 0.82 (95%CI, 0.78-0.87) to 0.88 (95%CI, 0.84-0.91), and decision curve analysis confirmed that its addition provided the highest net benefit.</p><p><strong>Conclusion: </strong>CRP adds value to history and physical examination when diagnosing appendicitis in children presenting acute abdominal pain in primary care. Appendicitis is least likely if the CRP value is < 10 mg/L and symptoms have been present for > 48 h.</p>","PeriodicalId":54380,"journal":{"name":"European Journal of General Practice","volume":"28 1","pages":"95-101"},"PeriodicalIF":2.3000,"publicationDate":"2022-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9103685/pdf/","citationCount":"0","resultStr":"{\"title\":\"Added value of CRP to clinical features when assessing appendicitis in children.\",\"authors\":\"Guus C G H Blok, Eelke D Nikkels, Johan van der Lei, Marjolein Y Berger, Gea A Holtman\",\"doi\":\"10.1080/13814788.2022.2067142\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The diagnostic value of C-reactive protein (CRP) for appendicitis in children has not been evaluated in primary care. As biochemical responses and differential diagnoses vary with age, separate evaluation in children and adults is needed.</p><p><strong>Objectives: </strong>To determine whether adding CRP to symptoms and signs improves the diagnosis of appendicitis in children with acute abdominal pain in primary care.</p><p><strong>Methods: </strong>A retrospective cohort study in Dutch general practice. Data was collected from the Integrated Primary Care Information database between 2010 and 2016. We included children aged 4-18 years, with no history of appendicitis, presenting with acute abdominal pain, and having a CRP test. Initial CRP levels were related to the specialist's diagnosis of appendicitis, and the test's characteristics were calculated for multiple cut-offs. The value of adding CRP to signs and symptoms was analysed by logistic regression.</p><p><strong>Results: </strong>We identified 1076 eligible children, among whom 203 were referred for specialist evaluation and 70 had appendicitis. The sensitivity and specificity of a CRP cut-off ≥10 mg/L were 0.87 (95%CI, 0.77-0.94) and 0.77 (95%CI, 0.74-0.79), respectively. When symptoms lasted > 48 h, this sensitivity increased to 1.00. Positive predictive values for CRP alone were low (0.18-0.38) for all cut-off values (6-100 mg/L). Adding CRP increased the area under the curve from 0.82 (95%CI, 0.78-0.87) to 0.88 (95%CI, 0.84-0.91), and decision curve analysis confirmed that its addition provided the highest net benefit.</p><p><strong>Conclusion: </strong>CRP adds value to history and physical examination when diagnosing appendicitis in children presenting acute abdominal pain in primary care. Appendicitis is least likely if the CRP value is < 10 mg/L and symptoms have been present for > 48 h.</p>\",\"PeriodicalId\":54380,\"journal\":{\"name\":\"European Journal of General Practice\",\"volume\":\"28 1\",\"pages\":\"95-101\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2022-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9103685/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Journal of General Practice\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1080/13814788.2022.2067142\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of General Practice","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1080/13814788.2022.2067142","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Added value of CRP to clinical features when assessing appendicitis in children.
Background: The diagnostic value of C-reactive protein (CRP) for appendicitis in children has not been evaluated in primary care. As biochemical responses and differential diagnoses vary with age, separate evaluation in children and adults is needed.
Objectives: To determine whether adding CRP to symptoms and signs improves the diagnosis of appendicitis in children with acute abdominal pain in primary care.
Methods: A retrospective cohort study in Dutch general practice. Data was collected from the Integrated Primary Care Information database between 2010 and 2016. We included children aged 4-18 years, with no history of appendicitis, presenting with acute abdominal pain, and having a CRP test. Initial CRP levels were related to the specialist's diagnosis of appendicitis, and the test's characteristics were calculated for multiple cut-offs. The value of adding CRP to signs and symptoms was analysed by logistic regression.
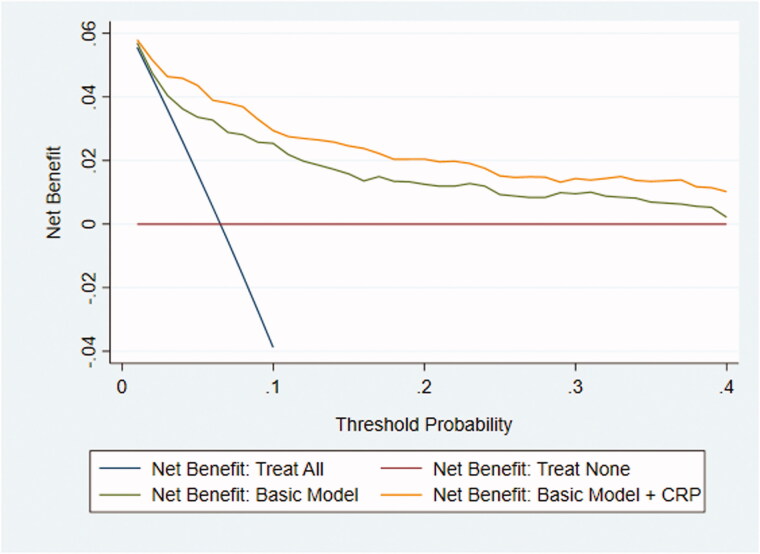
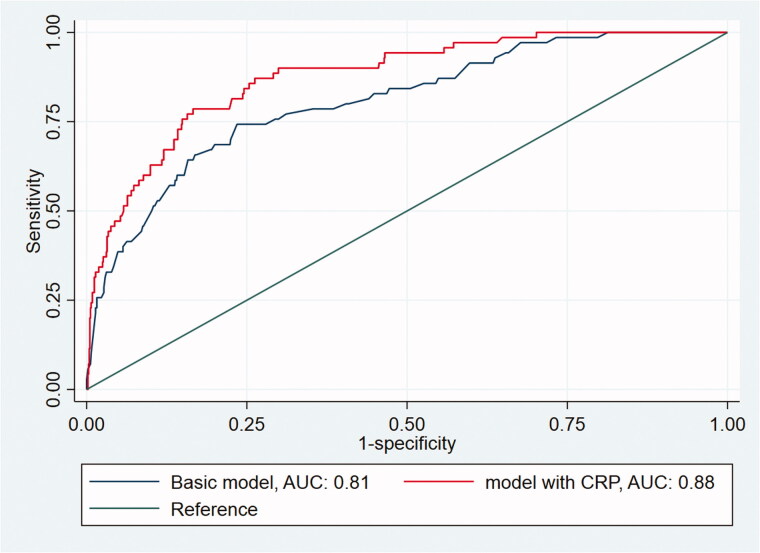
Results: We identified 1076 eligible children, among whom 203 were referred for specialist evaluation and 70 had appendicitis. The sensitivity and specificity of a CRP cut-off ≥10 mg/L were 0.87 (95%CI, 0.77-0.94) and 0.77 (95%CI, 0.74-0.79), respectively. When symptoms lasted > 48 h, this sensitivity increased to 1.00. Positive predictive values for CRP alone were low (0.18-0.38) for all cut-off values (6-100 mg/L). Adding CRP increased the area under the curve from 0.82 (95%CI, 0.78-0.87) to 0.88 (95%CI, 0.84-0.91), and decision curve analysis confirmed that its addition provided the highest net benefit.
Conclusion: CRP adds value to history and physical examination when diagnosing appendicitis in children presenting acute abdominal pain in primary care. Appendicitis is least likely if the CRP value is < 10 mg/L and symptoms have been present for > 48 h.
期刊介绍:
The EJGP aims to:
foster scientific research in primary care medicine (family medicine, general practice) in Europe
stimulate education and debate, relevant for the development of primary care medicine in Europe.
Scope
The EJGP publishes original research papers, review articles and clinical case reports on all aspects of primary care medicine (family medicine, general practice), providing new knowledge on medical decision-making, healthcare delivery, medical education, and research methodology.
Areas covered include primary care epidemiology, prevention, diagnosis, pharmacotherapy, non-drug interventions, multi- and comorbidity, palliative care, shared decision making, inter-professional collaboration, quality and safety, training and teaching, and quantitative and qualitative research methods.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


