Yi Liu, Yanguang Yang, Guomei Tai, Feng Ni, Cenming Yu, Wenjing Zhao, Ding Wang
{"title":"胃癌根治术患者术前血小板计数/(淋巴细胞计数×前白蛋白计数)比值与预后的关系","authors":"Yi Liu, Yanguang Yang, Guomei Tai, Feng Ni, Cenming Yu, Wenjing Zhao, Ding Wang","doi":"10.1155/2023/8401579","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To clarify the relationship between preoperative platelet count/(lymphocyte count × prealbumin count) ratio (PLPR) and the prognosis of patients with gastric cancer undergoing a radical operation, combined with Tumor Node Metastasis (TNM) staging, a scoring system was established to guide clinical application.</p><p><strong>Methods: </strong>The clinical data of 238 patients receiving radical operations for gastric cancer were retrospectively analyzed. According to the area under the Receiver operating characteristic curve, the predictive value of the preoperative PLPR for the 5-year overall survival (OS) of gastric cancer was determined, and the best cut-off value of the ratio was corresponding to the maximum value of Yoden index. Chi-squared test was applied to analyze the correlation between the ratio and clinicopathological features. Kaplan-Meier curve was applied to analyze the influence of this ratio on 5-year OS. The Cox regression model was applied to analyze the hazards affecting the long-term survival of patients. The nomogram model was used to predict the long-term survival rate.</p><p><strong>Results: </strong>The optimal cut-off point of preoperative PLPR ratio was 7.46, and the patients were segmented into two sets: one set of ratio <7.46 and another set of ratio ≥7.46. The ratio was correlated with the size of the tumor, T stage, N stage, total stage, vascular cancer thrombus, and nerve invasion. In stage I-III patients, the prognosis was better in the low-ratio set than in the high-ratio set (<i>P</i> < 0.001), subgroup analysis indicated the prognosis was obviously better in the low-ratio set than in the high-ratio set in stage II and III patients (<i>P</i> < 0.05 and <i>P</i> < 0.001), but there was no difference in stage I patients (<i>P</i> > 0.05). Age, T stage, N stage, total TNM stage, tumor size, vascular tumor thrombus, nerve invasion, preoperative neutrophil count/lymphocyte count (NLR; reference value 3.68), preoperative PLPR (reference value 7.46), preoperative platelet count/lymphocyte count (PLR; reference value 159.56), and preoperative platelet count × NLR (SII; reference value 915.48) were related to patient prognosis (<i>P</i> < 0.05); meanwhile age, total TNM stage, preoperative PLPR (reference value 7.46), preoperative PLR (reference value 159.56), and preoperative SII (reference value 915.48) were independent hazards for prognosis (<i>P</i> < 0.05). Five independent risk factors were analyzed by nomogram model to predict the 5-year OS of patients who underwent a radical operation for carcinoma of the stomach.</p><p><strong>Conclusion: </strong>Preoperative PLPR ratio (reference value 7.46) is an independent risk factor for long-term prognosis in patients undergoing a radical operation for gastric cancer. The nomogram scoring system established by postoperative TNM staging combined with this ratio and age, PLR, and SII can better forecast the survival of patients who underwent radical operation for carcinoma of the stomach.</p>","PeriodicalId":12597,"journal":{"name":"Gastroenterology Research and Practice","volume":"2023 ","pages":"8401579"},"PeriodicalIF":1.4000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10403323/pdf/","citationCount":"0","resultStr":"{\"title\":\"Correlation between Preoperative Platelet Count/(Lymphocyte Count × Prealbumin Count) Ratio and the Prognosis of Patients with Gastric Cancer Undergoing Radical Operation.\",\"authors\":\"Yi Liu, Yanguang Yang, Guomei Tai, Feng Ni, Cenming Yu, Wenjing Zhao, Ding Wang\",\"doi\":\"10.1155/2023/8401579\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To clarify the relationship between preoperative platelet count/(lymphocyte count × prealbumin count) ratio (PLPR) and the prognosis of patients with gastric cancer undergoing a radical operation, combined with Tumor Node Metastasis (TNM) staging, a scoring system was established to guide clinical application.</p><p><strong>Methods: </strong>The clinical data of 238 patients receiving radical operations for gastric cancer were retrospectively analyzed. According to the area under the Receiver operating characteristic curve, the predictive value of the preoperative PLPR for the 5-year overall survival (OS) of gastric cancer was determined, and the best cut-off value of the ratio was corresponding to the maximum value of Yoden index. Chi-squared test was applied to analyze the correlation between the ratio and clinicopathological features. Kaplan-Meier curve was applied to analyze the influence of this ratio on 5-year OS. The Cox regression model was applied to analyze the hazards affecting the long-term survival of patients. The nomogram model was used to predict the long-term survival rate.</p><p><strong>Results: </strong>The optimal cut-off point of preoperative PLPR ratio was 7.46, and the patients were segmented into two sets: one set of ratio <7.46 and another set of ratio ≥7.46. The ratio was correlated with the size of the tumor, T stage, N stage, total stage, vascular cancer thrombus, and nerve invasion. In stage I-III patients, the prognosis was better in the low-ratio set than in the high-ratio set (<i>P</i> < 0.001), subgroup analysis indicated the prognosis was obviously better in the low-ratio set than in the high-ratio set in stage II and III patients (<i>P</i> < 0.05 and <i>P</i> < 0.001), but there was no difference in stage I patients (<i>P</i> > 0.05). Age, T stage, N stage, total TNM stage, tumor size, vascular tumor thrombus, nerve invasion, preoperative neutrophil count/lymphocyte count (NLR; reference value 3.68), preoperative PLPR (reference value 7.46), preoperative platelet count/lymphocyte count (PLR; reference value 159.56), and preoperative platelet count × NLR (SII; reference value 915.48) were related to patient prognosis (<i>P</i> < 0.05); meanwhile age, total TNM stage, preoperative PLPR (reference value 7.46), preoperative PLR (reference value 159.56), and preoperative SII (reference value 915.48) were independent hazards for prognosis (<i>P</i> < 0.05). Five independent risk factors were analyzed by nomogram model to predict the 5-year OS of patients who underwent a radical operation for carcinoma of the stomach.</p><p><strong>Conclusion: </strong>Preoperative PLPR ratio (reference value 7.46) is an independent risk factor for long-term prognosis in patients undergoing a radical operation for gastric cancer. The nomogram scoring system established by postoperative TNM staging combined with this ratio and age, PLR, and SII can better forecast the survival of patients who underwent radical operation for carcinoma of the stomach.</p>\",\"PeriodicalId\":12597,\"journal\":{\"name\":\"Gastroenterology Research and Practice\",\"volume\":\"2023 \",\"pages\":\"8401579\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10403323/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Gastroenterology Research and Practice\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1155/2023/8401579\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Gastroenterology Research and Practice","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1155/2023/8401579","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Correlation between Preoperative Platelet Count/(Lymphocyte Count × Prealbumin Count) Ratio and the Prognosis of Patients with Gastric Cancer Undergoing Radical Operation.
Objective: To clarify the relationship between preoperative platelet count/(lymphocyte count × prealbumin count) ratio (PLPR) and the prognosis of patients with gastric cancer undergoing a radical operation, combined with Tumor Node Metastasis (TNM) staging, a scoring system was established to guide clinical application.
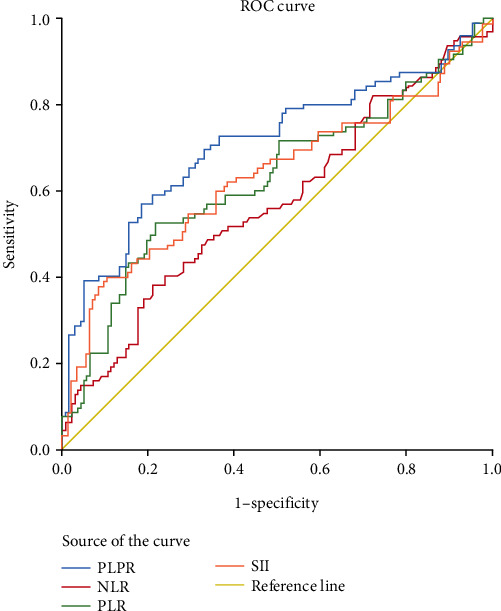
Methods: The clinical data of 238 patients receiving radical operations for gastric cancer were retrospectively analyzed. According to the area under the Receiver operating characteristic curve, the predictive value of the preoperative PLPR for the 5-year overall survival (OS) of gastric cancer was determined, and the best cut-off value of the ratio was corresponding to the maximum value of Yoden index. Chi-squared test was applied to analyze the correlation between the ratio and clinicopathological features. Kaplan-Meier curve was applied to analyze the influence of this ratio on 5-year OS. The Cox regression model was applied to analyze the hazards affecting the long-term survival of patients. The nomogram model was used to predict the long-term survival rate.
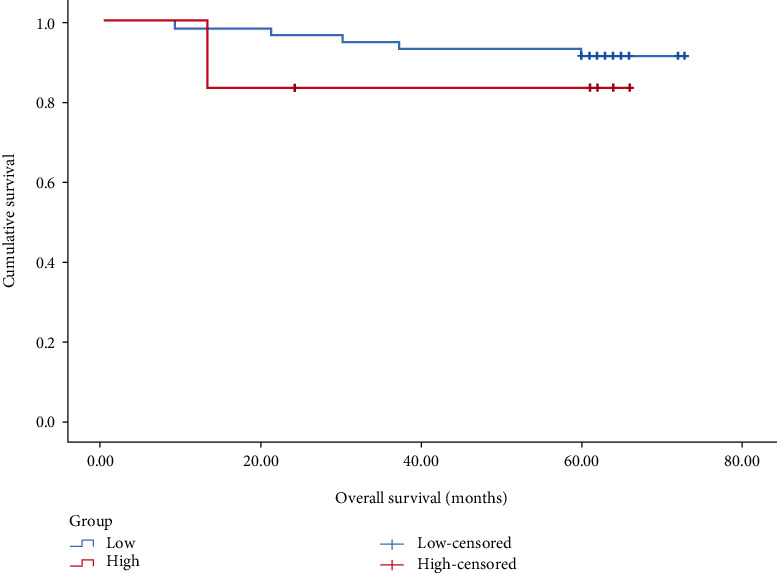
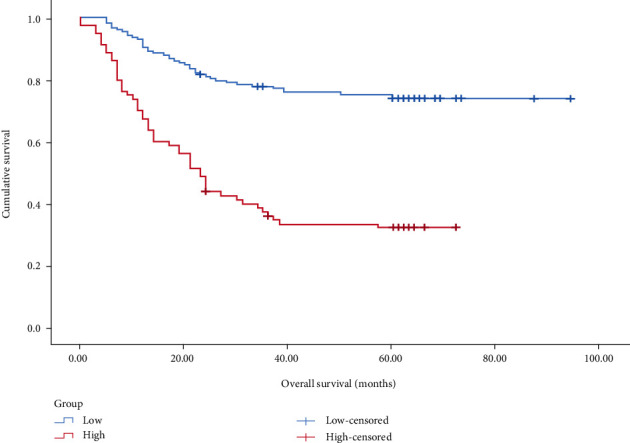
Results: The optimal cut-off point of preoperative PLPR ratio was 7.46, and the patients were segmented into two sets: one set of ratio <7.46 and another set of ratio ≥7.46. The ratio was correlated with the size of the tumor, T stage, N stage, total stage, vascular cancer thrombus, and nerve invasion. In stage I-III patients, the prognosis was better in the low-ratio set than in the high-ratio set (P < 0.001), subgroup analysis indicated the prognosis was obviously better in the low-ratio set than in the high-ratio set in stage II and III patients (P < 0.05 and P < 0.001), but there was no difference in stage I patients (P > 0.05). Age, T stage, N stage, total TNM stage, tumor size, vascular tumor thrombus, nerve invasion, preoperative neutrophil count/lymphocyte count (NLR; reference value 3.68), preoperative PLPR (reference value 7.46), preoperative platelet count/lymphocyte count (PLR; reference value 159.56), and preoperative platelet count × NLR (SII; reference value 915.48) were related to patient prognosis (P < 0.05); meanwhile age, total TNM stage, preoperative PLPR (reference value 7.46), preoperative PLR (reference value 159.56), and preoperative SII (reference value 915.48) were independent hazards for prognosis (P < 0.05). Five independent risk factors were analyzed by nomogram model to predict the 5-year OS of patients who underwent a radical operation for carcinoma of the stomach.
Conclusion: Preoperative PLPR ratio (reference value 7.46) is an independent risk factor for long-term prognosis in patients undergoing a radical operation for gastric cancer. The nomogram scoring system established by postoperative TNM staging combined with this ratio and age, PLR, and SII can better forecast the survival of patients who underwent radical operation for carcinoma of the stomach.
期刊介绍:
Gastroenterology Research and Practice is a peer-reviewed, Open Access journal which publishes original research articles, review articles and clinical studies based on all areas of gastroenterology, hepatology, pancreas and biliary, and related cancers. The journal welcomes submissions on the physiology, pathophysiology, etiology, diagnosis and therapy of gastrointestinal diseases. The aim of the journal is to provide cutting edge research related to the field of gastroenterology, as well as digestive diseases and disorders.
Topics of interest include:
Management of pancreatic diseases
Third space endoscopy
Endoscopic resection
Therapeutic endoscopy
Therapeutic endosonography.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


