{"title":"关于白蛋白治疗肝硬化的争议。","authors":"Jonel Trebicka, Guadalupe Garcia-Tsao","doi":"10.1097/HEP.0000000000000521","DOIUrl":null,"url":null,"abstract":"<p><p>Albumin is the most abundant protein in the human body and is synthetized exclusively by the liver. Therefore, serum albumin levels are reduced in acute and/or chronic liver disease. In cirrhosis, low levels of albumin predict the outcome. In advanced cirrhosis, the quality of albumin is decreased due to high oxidative stress and a proinflammatory state. Therefore, the administration of i.v. albumin would seem to be of pathophysiological relevance and benefit. Yet, the questions that remain are who, when, how much, and how often. While albumin infusion is recommended after large-volume paracentesis, at diagnosis of spontaneous bacterial peritonitis, in acute kidney injury, and in hepatorenal syndrome, the amount and schedule of albumin to be administered require refinement, particularly given complications related to volume overload that have become increasingly apparent. Other indications for albumin such as infections other than spontaneous bacterial peritonitis, hyponatremia, HE, prevention of poor outcomes in hospitalized, and in outpatients with cirrhosis are still debated. The results of studies in these settings are either negative, controversial, or inconclusive. This sheds some doubts regarding the use of albumin as a \"one size fits all\" strategy. The indication and patient selection are crucial and not always intuitive. The amount and frequency also seem to play a role in the success or failure of albumin. This review will critically discuss the evidence and underline areas where there are indications for albumin use and others where evidence is still insufficient and will have to await the development/results of randomized controlled trials.</p>","PeriodicalId":177,"journal":{"name":"Hepatology","volume":" ","pages":"288-303"},"PeriodicalIF":15.8000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11643133/pdf/","citationCount":"0","resultStr":"{\"title\":\"Controversies regarding albumin therapy in cirrhosis.\",\"authors\":\"Jonel Trebicka, Guadalupe Garcia-Tsao\",\"doi\":\"10.1097/HEP.0000000000000521\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Albumin is the most abundant protein in the human body and is synthetized exclusively by the liver. Therefore, serum albumin levels are reduced in acute and/or chronic liver disease. In cirrhosis, low levels of albumin predict the outcome. In advanced cirrhosis, the quality of albumin is decreased due to high oxidative stress and a proinflammatory state. Therefore, the administration of i.v. albumin would seem to be of pathophysiological relevance and benefit. Yet, the questions that remain are who, when, how much, and how often. While albumin infusion is recommended after large-volume paracentesis, at diagnosis of spontaneous bacterial peritonitis, in acute kidney injury, and in hepatorenal syndrome, the amount and schedule of albumin to be administered require refinement, particularly given complications related to volume overload that have become increasingly apparent. Other indications for albumin such as infections other than spontaneous bacterial peritonitis, hyponatremia, HE, prevention of poor outcomes in hospitalized, and in outpatients with cirrhosis are still debated. The results of studies in these settings are either negative, controversial, or inconclusive. This sheds some doubts regarding the use of albumin as a \\\"one size fits all\\\" strategy. The indication and patient selection are crucial and not always intuitive. The amount and frequency also seem to play a role in the success or failure of albumin. This review will critically discuss the evidence and underline areas where there are indications for albumin use and others where evidence is still insufficient and will have to await the development/results of randomized controlled trials.</p>\",\"PeriodicalId\":177,\"journal\":{\"name\":\"Hepatology\",\"volume\":\" \",\"pages\":\"288-303\"},\"PeriodicalIF\":15.8000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11643133/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Hepatology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1097/HEP.0000000000000521\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/8/7 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Hepatology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1097/HEP.0000000000000521","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/8/7 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Controversies regarding albumin therapy in cirrhosis.
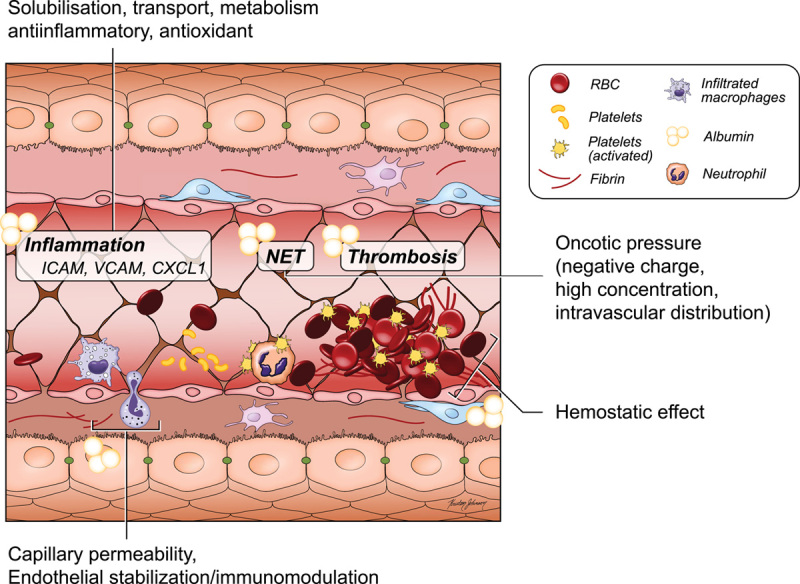
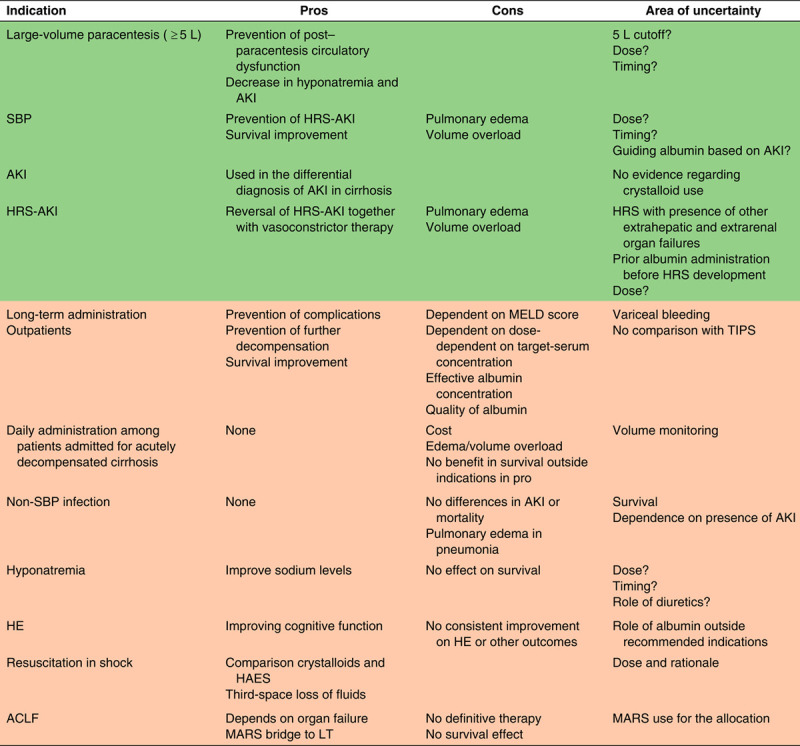
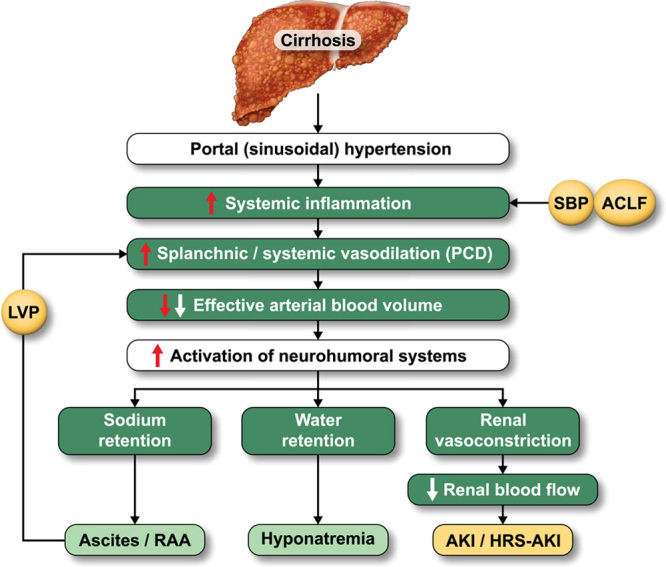
Albumin is the most abundant protein in the human body and is synthetized exclusively by the liver. Therefore, serum albumin levels are reduced in acute and/or chronic liver disease. In cirrhosis, low levels of albumin predict the outcome. In advanced cirrhosis, the quality of albumin is decreased due to high oxidative stress and a proinflammatory state. Therefore, the administration of i.v. albumin would seem to be of pathophysiological relevance and benefit. Yet, the questions that remain are who, when, how much, and how often. While albumin infusion is recommended after large-volume paracentesis, at diagnosis of spontaneous bacterial peritonitis, in acute kidney injury, and in hepatorenal syndrome, the amount and schedule of albumin to be administered require refinement, particularly given complications related to volume overload that have become increasingly apparent. Other indications for albumin such as infections other than spontaneous bacterial peritonitis, hyponatremia, HE, prevention of poor outcomes in hospitalized, and in outpatients with cirrhosis are still debated. The results of studies in these settings are either negative, controversial, or inconclusive. This sheds some doubts regarding the use of albumin as a "one size fits all" strategy. The indication and patient selection are crucial and not always intuitive. The amount and frequency also seem to play a role in the success or failure of albumin. This review will critically discuss the evidence and underline areas where there are indications for albumin use and others where evidence is still insufficient and will have to await the development/results of randomized controlled trials.
期刊介绍:
HEPATOLOGY is recognized as the leading publication in the field of liver disease. It features original, peer-reviewed articles covering various aspects of liver structure, function, and disease. The journal's distinguished Editorial Board carefully selects the best articles each month, focusing on topics including immunology, chronic hepatitis, viral hepatitis, cirrhosis, genetic and metabolic liver diseases, liver cancer, and drug metabolism.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


