Giacomo Calini, Mohamed A Abd El Aziz, Lucia Paolini, Solafah Abdalla, Matteo Rottoli, Giulio Mari, David W Larson
{"title":"症状性无并发症憩室病(SUDD):临床管理的实践指导和挑战。","authors":"Giacomo Calini, Mohamed A Abd El Aziz, Lucia Paolini, Solafah Abdalla, Matteo Rottoli, Giulio Mari, David W Larson","doi":"10.2147/CEG.S340929","DOIUrl":null,"url":null,"abstract":"<p><p>Symptomatic Uncomplicated Diverticular Disease (SUDD) is a syndrome within the diverticular disease spectrum, characterized by local abdominal pain with bowel movement changes but without systemic inflammation. This narrative review reports current knowledge, delivers practical guidance, and reveals challenges for the clinical management of SUDD. A broad and common consensus on the definition of SUDD is still needed. However, it is mainly considered a chronic condition that impairs quality of life (QoL) and is characterized by persistent left lower quadrant abdominal pain with bowel movement changes (eg, diarrhea) and low-grade inflammation (eg, elevated calprotectin) but without systemic inflammation. Age, genetic predisposition, obesity, physical inactivity, low-fiber diet, and smoking are considered risk factors. The pathogenesis of SUDD is not entirely clarified. It seems to result from an interaction between fecal microbiota alterations, neuro-immune enteric interactions, and muscular system dysfunction associated with a low-grade and local inflammatory state. At diagnosis, it is essential to assess baseline clinical and Quality of Life (QoL) scores to evaluate treatment efficacy and, ideally, to enroll patients in cohort studies, clinical trials, or registries. SUDD treatments aim to improve symptoms and QoL, prevent recurrence, and avoid disease progression and complications. An overall healthy lifestyle - physical activity and a high-fiber diet, with a focus on whole grains, fruits, and vegetables - is encouraged. Probiotics could effectively reduce symptoms in patients with SUDD, but their utility is missing adequate evidence. Using Rifaximin plus fiber and Mesalazine offers potential in controlling symptoms in patients with SUDD and might prevent acute diverticulitis. Surgery could be considered in patients with medical treatment failure and persistently impaired QoL. Still, studies with well-defined diagnostic criteria for SUDD that evaluate the safety, QoL, effectiveness, and cost-effectiveness of these interventions using standard scores and comparable outcomes are needed.</p>","PeriodicalId":10208,"journal":{"name":"Clinical and Experimental Gastroenterology","volume":"16 ","pages":"29-43"},"PeriodicalIF":2.3000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/81/e9/ceg-16-29.PMC10066719.pdf","citationCount":"2","resultStr":"{\"title\":\"Symptomatic Uncomplicated Diverticular Disease (SUDD): Practical Guidance and Challenges for Clinical Management.\",\"authors\":\"Giacomo Calini, Mohamed A Abd El Aziz, Lucia Paolini, Solafah Abdalla, Matteo Rottoli, Giulio Mari, David W Larson\",\"doi\":\"10.2147/CEG.S340929\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Symptomatic Uncomplicated Diverticular Disease (SUDD) is a syndrome within the diverticular disease spectrum, characterized by local abdominal pain with bowel movement changes but without systemic inflammation. This narrative review reports current knowledge, delivers practical guidance, and reveals challenges for the clinical management of SUDD. A broad and common consensus on the definition of SUDD is still needed. However, it is mainly considered a chronic condition that impairs quality of life (QoL) and is characterized by persistent left lower quadrant abdominal pain with bowel movement changes (eg, diarrhea) and low-grade inflammation (eg, elevated calprotectin) but without systemic inflammation. Age, genetic predisposition, obesity, physical inactivity, low-fiber diet, and smoking are considered risk factors. The pathogenesis of SUDD is not entirely clarified. It seems to result from an interaction between fecal microbiota alterations, neuro-immune enteric interactions, and muscular system dysfunction associated with a low-grade and local inflammatory state. At diagnosis, it is essential to assess baseline clinical and Quality of Life (QoL) scores to evaluate treatment efficacy and, ideally, to enroll patients in cohort studies, clinical trials, or registries. SUDD treatments aim to improve symptoms and QoL, prevent recurrence, and avoid disease progression and complications. An overall healthy lifestyle - physical activity and a high-fiber diet, with a focus on whole grains, fruits, and vegetables - is encouraged. Probiotics could effectively reduce symptoms in patients with SUDD, but their utility is missing adequate evidence. Using Rifaximin plus fiber and Mesalazine offers potential in controlling symptoms in patients with SUDD and might prevent acute diverticulitis. Surgery could be considered in patients with medical treatment failure and persistently impaired QoL. Still, studies with well-defined diagnostic criteria for SUDD that evaluate the safety, QoL, effectiveness, and cost-effectiveness of these interventions using standard scores and comparable outcomes are needed.</p>\",\"PeriodicalId\":10208,\"journal\":{\"name\":\"Clinical and Experimental Gastroenterology\",\"volume\":\"16 \",\"pages\":\"29-43\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/81/e9/ceg-16-29.PMC10066719.pdf\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical and Experimental Gastroenterology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/CEG.S340929\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Experimental Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/CEG.S340929","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Symptomatic Uncomplicated Diverticular Disease (SUDD): Practical Guidance and Challenges for Clinical Management.
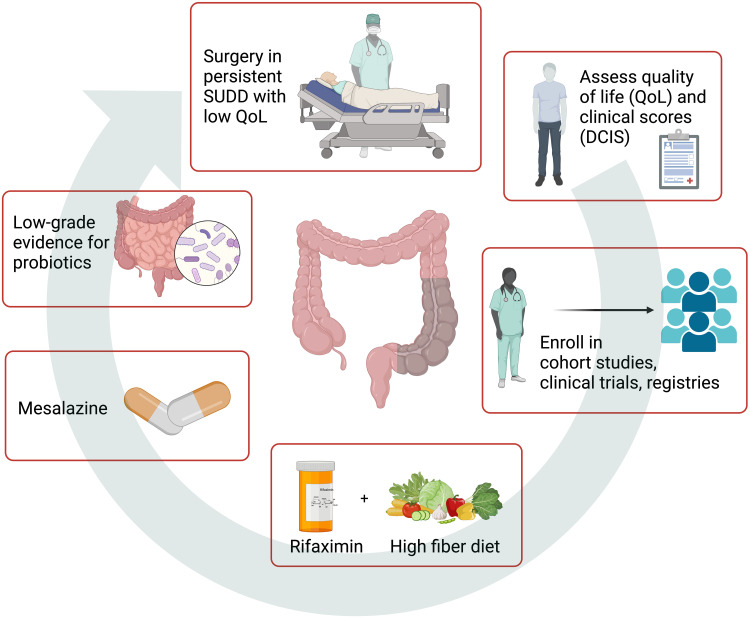
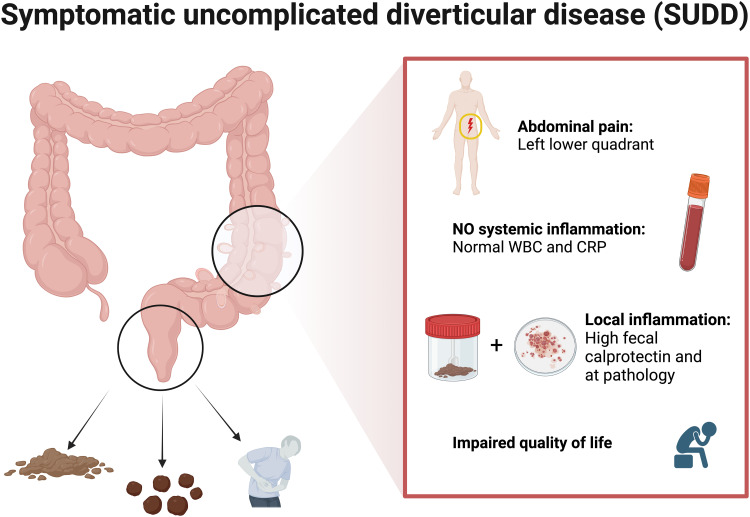
Symptomatic Uncomplicated Diverticular Disease (SUDD) is a syndrome within the diverticular disease spectrum, characterized by local abdominal pain with bowel movement changes but without systemic inflammation. This narrative review reports current knowledge, delivers practical guidance, and reveals challenges for the clinical management of SUDD. A broad and common consensus on the definition of SUDD is still needed. However, it is mainly considered a chronic condition that impairs quality of life (QoL) and is characterized by persistent left lower quadrant abdominal pain with bowel movement changes (eg, diarrhea) and low-grade inflammation (eg, elevated calprotectin) but without systemic inflammation. Age, genetic predisposition, obesity, physical inactivity, low-fiber diet, and smoking are considered risk factors. The pathogenesis of SUDD is not entirely clarified. It seems to result from an interaction between fecal microbiota alterations, neuro-immune enteric interactions, and muscular system dysfunction associated with a low-grade and local inflammatory state. At diagnosis, it is essential to assess baseline clinical and Quality of Life (QoL) scores to evaluate treatment efficacy and, ideally, to enroll patients in cohort studies, clinical trials, or registries. SUDD treatments aim to improve symptoms and QoL, prevent recurrence, and avoid disease progression and complications. An overall healthy lifestyle - physical activity and a high-fiber diet, with a focus on whole grains, fruits, and vegetables - is encouraged. Probiotics could effectively reduce symptoms in patients with SUDD, but their utility is missing adequate evidence. Using Rifaximin plus fiber and Mesalazine offers potential in controlling symptoms in patients with SUDD and might prevent acute diverticulitis. Surgery could be considered in patients with medical treatment failure and persistently impaired QoL. Still, studies with well-defined diagnostic criteria for SUDD that evaluate the safety, QoL, effectiveness, and cost-effectiveness of these interventions using standard scores and comparable outcomes are needed.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


