Polona Gams, Marko Bitenc, Nenad Danojevic, Tomaz Jensterle, Aleksander Sadikov, Vida Groznik, Maja Sostaric
{"title":"竖脊肌平面阻滞与肋间神经阻滞在肺癌术后镇痛中的应用。","authors":"Polona Gams, Marko Bitenc, Nenad Danojevic, Tomaz Jensterle, Aleksander Sadikov, Vida Groznik, Maja Sostaric","doi":"10.2478/raon-2023-0035","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>A recent trend in postoperative analgesia for lung cancer surgery relies on regional nerve blocks with decreased opioid administration. Our study aims to critically assess the continuous ultrasound-guided <i>erector spinae</i> plane block (ESPB) at our institution and compare it to a standard regional anesthetic technique, the intercostal nerve block (ICNB).</p><p><strong>Patients and methods: </strong>A prospective randomized-control study was performed to compare outcomes of patients, scheduled for video-assisted thoracoscopic (VATS) lung cancer resection, allocated to the ESPB or ICNB group. Primary outcomes were total opioid consumption and subjective pain scores at rest and cough each hour in 48 h after surgery. The secondary outcome was respiratory muscle strength, measured by maximal inspiratory and expiratory pressures (MIP/MEP) after 24 h and 48 h.</p><p><strong>Results: </strong>60 patients met the inclusion criteria, half ESPB. Total opioid consumption in the first 48 h was 21. 64 ± 14.22 mg in the ESPB group and 38.34 ± 29.91 mg in the ICNB group (p = 0.035). The patients in the ESPB group had lower numerical rating scores at rest than in the ICNB group (1.19 ± 0.73 <i>vs.</i> 1.77 ± 1.01, p = 0.039). There were no significant differences in MIP/MEP decrease from baseline after 24 h (MIP p = 0.088, MEP p = 0.182) or 48 h (MIP p = 0.110, MEP p = 0.645), time to chest tube removal or hospital discharge between the two groups.</p><p><strong>Conclusions: </strong>In the first 48 h after surgery, patients with continuous ESPB required fewer opioids and reported less pain than patients with ICNB. There were no differences regarding respiratory muscle strength, postoperative complications, and time to hospital discharge. In addition, continuous ESPB demanded more surveillance than ICNB.</p>","PeriodicalId":21034,"journal":{"name":"Radiology and Oncology","volume":"57 3","pages":"364-370"},"PeriodicalIF":2.1000,"publicationDate":"2023-09-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10476902/pdf/","citationCount":"1","resultStr":"{\"title\":\"Erector spinae plane block versus intercostal nerve block for postoperative analgesia in lung cancer surgery.\",\"authors\":\"Polona Gams, Marko Bitenc, Nenad Danojevic, Tomaz Jensterle, Aleksander Sadikov, Vida Groznik, Maja Sostaric\",\"doi\":\"10.2478/raon-2023-0035\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>A recent trend in postoperative analgesia for lung cancer surgery relies on regional nerve blocks with decreased opioid administration. Our study aims to critically assess the continuous ultrasound-guided <i>erector spinae</i> plane block (ESPB) at our institution and compare it to a standard regional anesthetic technique, the intercostal nerve block (ICNB).</p><p><strong>Patients and methods: </strong>A prospective randomized-control study was performed to compare outcomes of patients, scheduled for video-assisted thoracoscopic (VATS) lung cancer resection, allocated to the ESPB or ICNB group. Primary outcomes were total opioid consumption and subjective pain scores at rest and cough each hour in 48 h after surgery. The secondary outcome was respiratory muscle strength, measured by maximal inspiratory and expiratory pressures (MIP/MEP) after 24 h and 48 h.</p><p><strong>Results: </strong>60 patients met the inclusion criteria, half ESPB. Total opioid consumption in the first 48 h was 21. 64 ± 14.22 mg in the ESPB group and 38.34 ± 29.91 mg in the ICNB group (p = 0.035). The patients in the ESPB group had lower numerical rating scores at rest than in the ICNB group (1.19 ± 0.73 <i>vs.</i> 1.77 ± 1.01, p = 0.039). There were no significant differences in MIP/MEP decrease from baseline after 24 h (MIP p = 0.088, MEP p = 0.182) or 48 h (MIP p = 0.110, MEP p = 0.645), time to chest tube removal or hospital discharge between the two groups.</p><p><strong>Conclusions: </strong>In the first 48 h after surgery, patients with continuous ESPB required fewer opioids and reported less pain than patients with ICNB. There were no differences regarding respiratory muscle strength, postoperative complications, and time to hospital discharge. In addition, continuous ESPB demanded more surveillance than ICNB.</p>\",\"PeriodicalId\":21034,\"journal\":{\"name\":\"Radiology and Oncology\",\"volume\":\"57 3\",\"pages\":\"364-370\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2023-09-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10476902/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Radiology and Oncology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.2478/raon-2023-0035\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/9/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Radiology and Oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2478/raon-2023-0035","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/9/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 1
摘要
背景:最近肺癌手术后镇痛的趋势依赖于减少阿片类药物给药的区域神经阻滞。我们的研究旨在批判性地评估我们机构的连续超声引导直立脊柱平面阻滞(ESPB),并将其与标准的区域麻醉技术肋间神经阻滞(ICNB)进行比较。患者和方法:进行了一项前瞻性随机对照研究,比较了计划进行视频胸腔镜(VATS)肺癌切除术的患者,分配到ESPB组或ICNB组的结果。主要结局是阿片类药物的总消耗和术后48小时休息和咳嗽时每小时的主观疼痛评分。次要终点是呼吸肌力量,通过24 h和48 h后的最大吸气和呼气压(MIP/MEP)测量。结果:60例患者符合纳入标准,一半为ESPB。前48小时阿片类药物总消耗量为21。ESPB组为64±14.22 mg, ICNB组为38.34±29.91 mg (p = 0.035)。ESPB组患者休息时的数值评分低于ICNB组(1.19±0.73比1.77±1.01,p = 0.039)。两组患者在24 h (MIP p = 0.088, MEP = 0.182)、48 h (MIP p = 0.110, MEP = 0.645)、拔胸管时间和出院时间较基线的MIP/MEP下降无显著差异。结论:在术后48小时内,持续ESPB患者比ICNB患者需要更少的阿片类药物,并且报告的疼痛更少。在呼吸肌力量、术后并发症和出院时间方面没有差异。此外,持续的ESPB需要比ICNB更多的监测。
Erector spinae plane block versus intercostal nerve block for postoperative analgesia in lung cancer surgery.
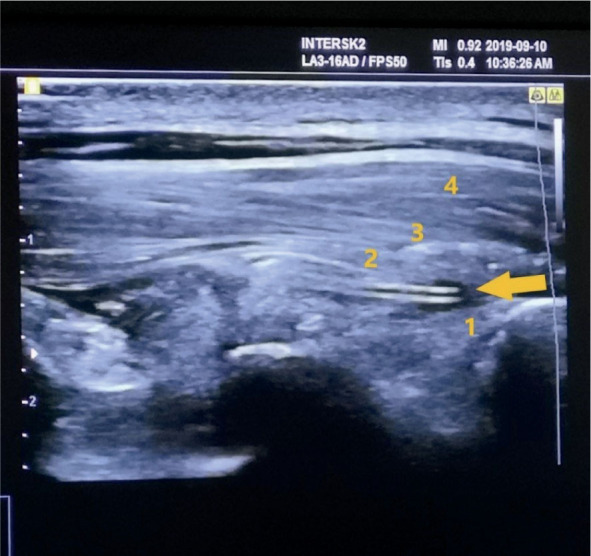
Background: A recent trend in postoperative analgesia for lung cancer surgery relies on regional nerve blocks with decreased opioid administration. Our study aims to critically assess the continuous ultrasound-guided erector spinae plane block (ESPB) at our institution and compare it to a standard regional anesthetic technique, the intercostal nerve block (ICNB).
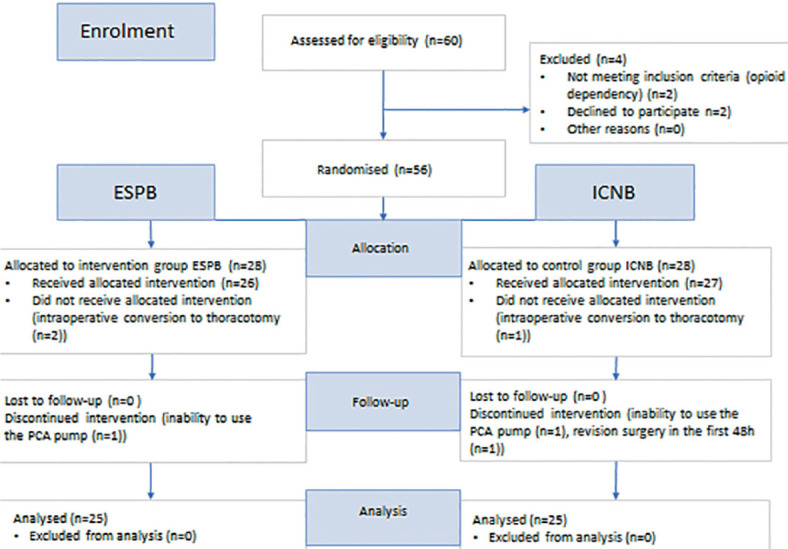
Patients and methods: A prospective randomized-control study was performed to compare outcomes of patients, scheduled for video-assisted thoracoscopic (VATS) lung cancer resection, allocated to the ESPB or ICNB group. Primary outcomes were total opioid consumption and subjective pain scores at rest and cough each hour in 48 h after surgery. The secondary outcome was respiratory muscle strength, measured by maximal inspiratory and expiratory pressures (MIP/MEP) after 24 h and 48 h.
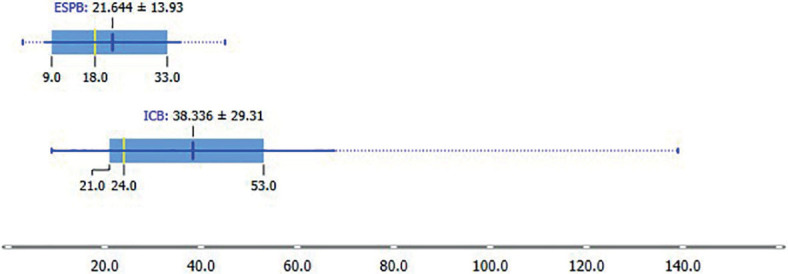
Results: 60 patients met the inclusion criteria, half ESPB. Total opioid consumption in the first 48 h was 21. 64 ± 14.22 mg in the ESPB group and 38.34 ± 29.91 mg in the ICNB group (p = 0.035). The patients in the ESPB group had lower numerical rating scores at rest than in the ICNB group (1.19 ± 0.73 vs. 1.77 ± 1.01, p = 0.039). There were no significant differences in MIP/MEP decrease from baseline after 24 h (MIP p = 0.088, MEP p = 0.182) or 48 h (MIP p = 0.110, MEP p = 0.645), time to chest tube removal or hospital discharge between the two groups.
Conclusions: In the first 48 h after surgery, patients with continuous ESPB required fewer opioids and reported less pain than patients with ICNB. There were no differences regarding respiratory muscle strength, postoperative complications, and time to hospital discharge. In addition, continuous ESPB demanded more surveillance than ICNB.
期刊介绍:
Radiology and Oncology is a multidisciplinary journal devoted to the publishing original and high quality scientific papers and review articles, pertinent to diagnostic and interventional radiology, computerized tomography, magnetic resonance, ultrasound, nuclear medicine, radiotherapy, clinical and experimental oncology, radiobiology, medical physics and radiation protection. Therefore, the scope of the journal is to cover beside radiology the diagnostic and therapeutic aspects in oncology, which distinguishes it from other journals in the field.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


