Annabelle M Warren, Mathis Grossmann, Mirjam Christ-Crain, Nicholas Russell
{"title":"不适当抗利尿综合征:从病理生理到治疗。","authors":"Annabelle M Warren, Mathis Grossmann, Mirjam Christ-Crain, Nicholas Russell","doi":"10.1210/endrev/bnad010","DOIUrl":null,"url":null,"abstract":"<p><p>Hyponatremia is the most common electrolyte disorder, affecting more than 15% of patients in the hospital. Syndrome of inappropriate antidiuresis (SIAD) is the most frequent cause of hypotonic hyponatremia, mediated by nonosmotic release of arginine vasopressin (AVP, previously known as antidiuretic hormone), which acts on the renal V2 receptors to promote water retention. There are a variety of underlying causes of SIAD, including malignancy, pulmonary pathology, and central nervous system pathology. In clinical practice, the etiology of hyponatremia is frequently multifactorial and the management approach may need to evolve during treatment of a single episode. It is therefore important to regularly reassess clinical status and biochemistry, while remaining alert to potential underlying etiological factors that may become more apparent during the course of treatment. In the absence of severe symptoms requiring urgent intervention, fluid restriction (FR) is widely endorsed as the first-line treatment for SIAD in current guidelines, but there is considerable controversy regarding second-line therapy in instances where FR is unsuccessful, which occurs in around half of cases. We review the epidemiology, pathophysiology, and differential diagnosis of SIAD, and summarize recent evidence for therapeutic options beyond FR, with a focus on tolvaptan, urea, and sodium-glucose cotransporter 2 inhibitors.</p>","PeriodicalId":11544,"journal":{"name":"Endocrine reviews","volume":"44 5","pages":"819-861"},"PeriodicalIF":22.0000,"publicationDate":"2023-09-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10502587/pdf/","citationCount":"3","resultStr":"{\"title\":\"Syndrome of Inappropriate Antidiuresis: From Pathophysiology to Management.\",\"authors\":\"Annabelle M Warren, Mathis Grossmann, Mirjam Christ-Crain, Nicholas Russell\",\"doi\":\"10.1210/endrev/bnad010\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Hyponatremia is the most common electrolyte disorder, affecting more than 15% of patients in the hospital. Syndrome of inappropriate antidiuresis (SIAD) is the most frequent cause of hypotonic hyponatremia, mediated by nonosmotic release of arginine vasopressin (AVP, previously known as antidiuretic hormone), which acts on the renal V2 receptors to promote water retention. There are a variety of underlying causes of SIAD, including malignancy, pulmonary pathology, and central nervous system pathology. In clinical practice, the etiology of hyponatremia is frequently multifactorial and the management approach may need to evolve during treatment of a single episode. It is therefore important to regularly reassess clinical status and biochemistry, while remaining alert to potential underlying etiological factors that may become more apparent during the course of treatment. In the absence of severe symptoms requiring urgent intervention, fluid restriction (FR) is widely endorsed as the first-line treatment for SIAD in current guidelines, but there is considerable controversy regarding second-line therapy in instances where FR is unsuccessful, which occurs in around half of cases. We review the epidemiology, pathophysiology, and differential diagnosis of SIAD, and summarize recent evidence for therapeutic options beyond FR, with a focus on tolvaptan, urea, and sodium-glucose cotransporter 2 inhibitors.</p>\",\"PeriodicalId\":11544,\"journal\":{\"name\":\"Endocrine reviews\",\"volume\":\"44 5\",\"pages\":\"819-861\"},\"PeriodicalIF\":22.0000,\"publicationDate\":\"2023-09-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10502587/pdf/\",\"citationCount\":\"3\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Endocrine reviews\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1210/endrev/bnad010\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Endocrine reviews","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1210/endrev/bnad010","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
Syndrome of Inappropriate Antidiuresis: From Pathophysiology to Management.
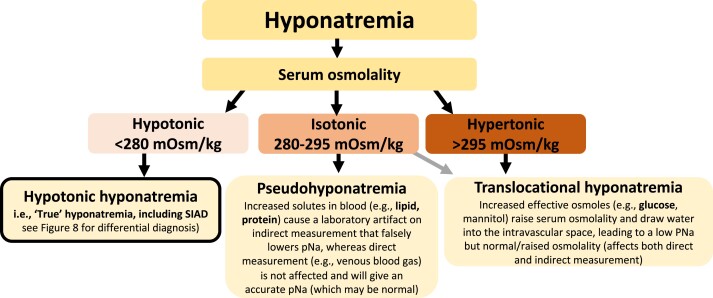
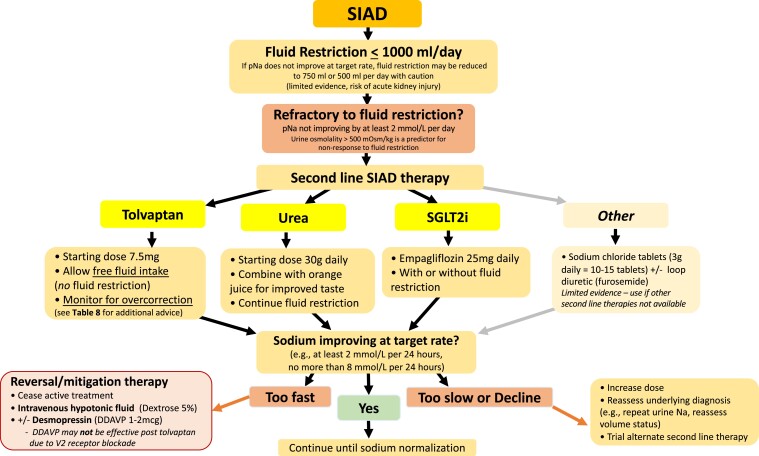
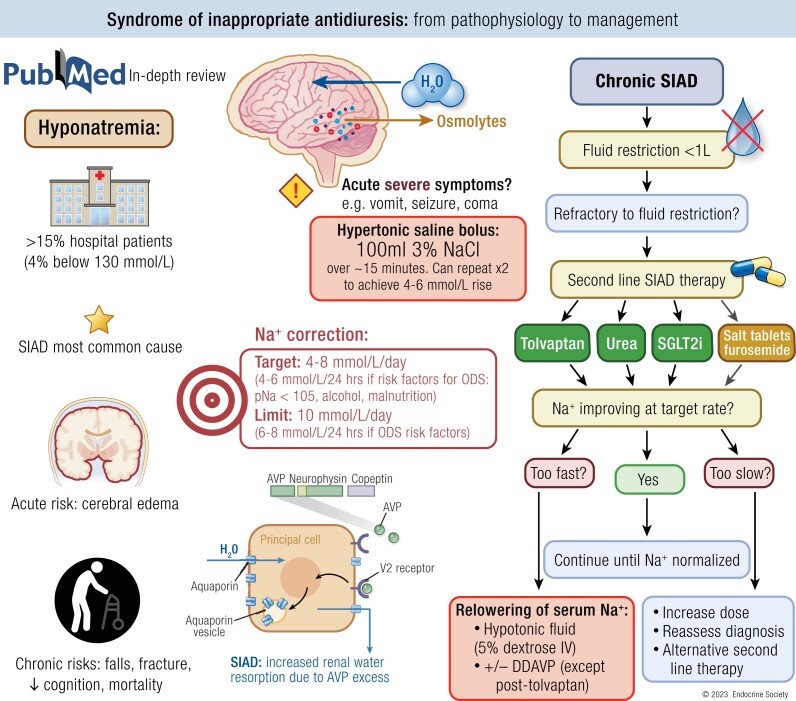
Hyponatremia is the most common electrolyte disorder, affecting more than 15% of patients in the hospital. Syndrome of inappropriate antidiuresis (SIAD) is the most frequent cause of hypotonic hyponatremia, mediated by nonosmotic release of arginine vasopressin (AVP, previously known as antidiuretic hormone), which acts on the renal V2 receptors to promote water retention. There are a variety of underlying causes of SIAD, including malignancy, pulmonary pathology, and central nervous system pathology. In clinical practice, the etiology of hyponatremia is frequently multifactorial and the management approach may need to evolve during treatment of a single episode. It is therefore important to regularly reassess clinical status and biochemistry, while remaining alert to potential underlying etiological factors that may become more apparent during the course of treatment. In the absence of severe symptoms requiring urgent intervention, fluid restriction (FR) is widely endorsed as the first-line treatment for SIAD in current guidelines, but there is considerable controversy regarding second-line therapy in instances where FR is unsuccessful, which occurs in around half of cases. We review the epidemiology, pathophysiology, and differential diagnosis of SIAD, and summarize recent evidence for therapeutic options beyond FR, with a focus on tolvaptan, urea, and sodium-glucose cotransporter 2 inhibitors.
期刊介绍:
Endocrine Reviews, published bimonthly, features concise timely reviews updating key mechanistic and clinical concepts, alongside comprehensive, authoritative articles covering both experimental and clinical endocrinology themes. The journal considers topics informing clinical practice based on emerging and established evidence from clinical research. It also reviews advances in endocrine science stemming from studies in cell biology, immunology, pharmacology, genetics, molecular biology, neuroscience, reproductive medicine, and pediatric endocrinology.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


