P Kissoonsingh, B Sutton, Syed U Iqbal, Lalit Pallan, Neil Steven, L Khoja
{"title":"黑色素瘤患者辅助抗pd -1免疫检查点抑制剂治疗继发嗜酸性哮喘","authors":"P Kissoonsingh, B Sutton, Syed U Iqbal, Lalit Pallan, Neil Steven, L Khoja","doi":"10.1155/2022/2658136","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Adjuvant immune checkpoint inhibitors are a new standard of care in melanoma. However, the immune related toxicity associated with these agents can be serious, and the long-term implications are yet to be defined especially in the adjuvant setting. We report, to our knowledge, the first case of anti-PD-1-induced eosinophilic asthma in a melanoma patient treated with adjuvant pembrolizumab. <i>Case Presentation.</i> A 72-year-old man commenced pembrolizumab in the adjuvant setting after resection of a stage IIIB cutaneous melanoma. The patient experienced episodes of breathlessness 4 weeks after cycle 1. These episodes were nocturnal and caused acute respiratory distress and cough, occasionally waking him up. The episodes progressed, and he was admitted after cycle 2 with a productive cough, wheeze, and breathlessness. Observations showed saturations on air of 94% and a respiratory rate of 19/min. The only laboratory abnormality was a raised eosinophil count of 1.1 × 10<sup>9</sup>. Spirometry showed a FEV1 of 2.57 (91% predicted), FVC of 4.04 (108% predicted), and ratio of 64%. Peak expiratory flow rate was 94% predicted, and corrected gas transfer was 6.29 (78% predicted) with KCO 1.18 (93% predicted). FeNO was raised at 129 indicating inflammation of his airways, and peak flow was 422 l/min. CT of the chest did not show pneumonitis or other lung pathology. A diagnosis of acute eosinophilic asthma was made. Treatment with steroids and beclometasone dipropionate and formoterol inhaler produced rapid resolution of symptoms and normalisation of the eosinophil count. Pembrolizumab was safely recommenced once steroids had discontinued and symptoms had resolved.</p><p><strong>Conclusions: </strong>Specialist respiratory input was needed for optimal patient management and is ongoing. Although a safe rechallenge with pembrolizumab was possible, treatment in the adjuvant setting is curative in intent and long-term safety follow-up is required to assess for delayed toxicity and long-term health implications. This is likely to require large regional/national/international databases to detect, monitor, and educate the wider medical community as these patients are followed up in primary care following initial specialist follow-up.</p>","PeriodicalId":9636,"journal":{"name":"Case Reports in Oncological Medicine","volume":"2022 ","pages":"2658136"},"PeriodicalIF":0.6000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9078828/pdf/","citationCount":"5","resultStr":"{\"title\":\"Eosinophilic Asthma Secondary to Adjuvant Anti-PD-1 Immune Checkpoint Inhibitor Treatment in a Melanoma Patient.\",\"authors\":\"P Kissoonsingh, B Sutton, Syed U Iqbal, Lalit Pallan, Neil Steven, L Khoja\",\"doi\":\"10.1155/2022/2658136\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Adjuvant immune checkpoint inhibitors are a new standard of care in melanoma. However, the immune related toxicity associated with these agents can be serious, and the long-term implications are yet to be defined especially in the adjuvant setting. We report, to our knowledge, the first case of anti-PD-1-induced eosinophilic asthma in a melanoma patient treated with adjuvant pembrolizumab. <i>Case Presentation.</i> A 72-year-old man commenced pembrolizumab in the adjuvant setting after resection of a stage IIIB cutaneous melanoma. The patient experienced episodes of breathlessness 4 weeks after cycle 1. These episodes were nocturnal and caused acute respiratory distress and cough, occasionally waking him up. The episodes progressed, and he was admitted after cycle 2 with a productive cough, wheeze, and breathlessness. Observations showed saturations on air of 94% and a respiratory rate of 19/min. The only laboratory abnormality was a raised eosinophil count of 1.1 × 10<sup>9</sup>. Spirometry showed a FEV1 of 2.57 (91% predicted), FVC of 4.04 (108% predicted), and ratio of 64%. Peak expiratory flow rate was 94% predicted, and corrected gas transfer was 6.29 (78% predicted) with KCO 1.18 (93% predicted). FeNO was raised at 129 indicating inflammation of his airways, and peak flow was 422 l/min. CT of the chest did not show pneumonitis or other lung pathology. A diagnosis of acute eosinophilic asthma was made. Treatment with steroids and beclometasone dipropionate and formoterol inhaler produced rapid resolution of symptoms and normalisation of the eosinophil count. Pembrolizumab was safely recommenced once steroids had discontinued and symptoms had resolved.</p><p><strong>Conclusions: </strong>Specialist respiratory input was needed for optimal patient management and is ongoing. Although a safe rechallenge with pembrolizumab was possible, treatment in the adjuvant setting is curative in intent and long-term safety follow-up is required to assess for delayed toxicity and long-term health implications. This is likely to require large regional/national/international databases to detect, monitor, and educate the wider medical community as these patients are followed up in primary care following initial specialist follow-up.</p>\",\"PeriodicalId\":9636,\"journal\":{\"name\":\"Case Reports in Oncological Medicine\",\"volume\":\"2022 \",\"pages\":\"2658136\"},\"PeriodicalIF\":0.6000,\"publicationDate\":\"2022-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9078828/pdf/\",\"citationCount\":\"5\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Oncological Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2022/2658136\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Oncological Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2022/2658136","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
Eosinophilic Asthma Secondary to Adjuvant Anti-PD-1 Immune Checkpoint Inhibitor Treatment in a Melanoma Patient.
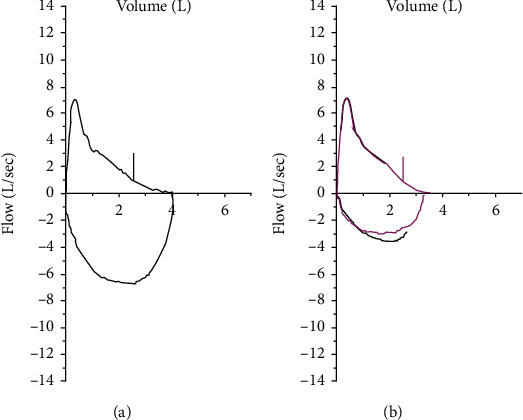
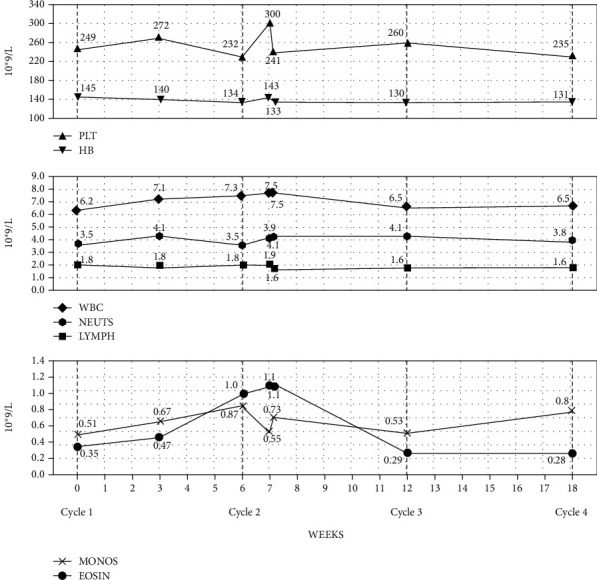
Background: Adjuvant immune checkpoint inhibitors are a new standard of care in melanoma. However, the immune related toxicity associated with these agents can be serious, and the long-term implications are yet to be defined especially in the adjuvant setting. We report, to our knowledge, the first case of anti-PD-1-induced eosinophilic asthma in a melanoma patient treated with adjuvant pembrolizumab. Case Presentation. A 72-year-old man commenced pembrolizumab in the adjuvant setting after resection of a stage IIIB cutaneous melanoma. The patient experienced episodes of breathlessness 4 weeks after cycle 1. These episodes were nocturnal and caused acute respiratory distress and cough, occasionally waking him up. The episodes progressed, and he was admitted after cycle 2 with a productive cough, wheeze, and breathlessness. Observations showed saturations on air of 94% and a respiratory rate of 19/min. The only laboratory abnormality was a raised eosinophil count of 1.1 × 109. Spirometry showed a FEV1 of 2.57 (91% predicted), FVC of 4.04 (108% predicted), and ratio of 64%. Peak expiratory flow rate was 94% predicted, and corrected gas transfer was 6.29 (78% predicted) with KCO 1.18 (93% predicted). FeNO was raised at 129 indicating inflammation of his airways, and peak flow was 422 l/min. CT of the chest did not show pneumonitis or other lung pathology. A diagnosis of acute eosinophilic asthma was made. Treatment with steroids and beclometasone dipropionate and formoterol inhaler produced rapid resolution of symptoms and normalisation of the eosinophil count. Pembrolizumab was safely recommenced once steroids had discontinued and symptoms had resolved.
Conclusions: Specialist respiratory input was needed for optimal patient management and is ongoing. Although a safe rechallenge with pembrolizumab was possible, treatment in the adjuvant setting is curative in intent and long-term safety follow-up is required to assess for delayed toxicity and long-term health implications. This is likely to require large regional/national/international databases to detect, monitor, and educate the wider medical community as these patients are followed up in primary care following initial specialist follow-up.
期刊介绍:
Case Reports in Oncological Medicine is a peer-reviewed, Open Access journal that publishes case reports and case series related to breast cancer, lung cancer, gastrointestinal cancer, skin cancer, head and neck cancer, paediatric oncology, neurooncology as well as genitourinary cancer.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


