Dani Rotman, Jorge Rojas Lievano, Shawn W O'Driscoll
{"title":"肘关节后外侧旋转不稳复发性后小头缺损的修复。","authors":"Dani Rotman, Jorge Rojas Lievano, Shawn W O'Driscoll","doi":"10.5397/cise.2022.01424","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Posterolateral rotatory instability (PLRI) is a common mechanism of recurrent elbow instability. While the essential lesion is a deficiency in the lateral ulnar collateral ligament (LUCL), there are often associated concomitant bony lesions, such as an Osborne-Cotterill lesions (posterior capitellar fractures) and marginal radial head fractures, that compromise stability. Currently, there is no standard treatment for posterior capitellar deficiency associated with recurrent PLRI.</p><p><strong>Methods: </strong>We conducted a retrospective review of five patients with recurrent PLRI of the elbow associated with a posterior capitellar impaction fracture engaging with the radial head during normal range of motion. The patients were treated surgically with LUCL reconstruction or repair and off-label reconstruction of the capitellar joint surface using a small metal prosthesis designed for metatarsal head resurfacing (HemiCAP toe classic).</p><p><strong>Results: </strong>Five patients (three adolescent males, two adult females) were treated between 2007 and 2018. At a median follow-up of 5 years, all patients had complete relief of their symptomatic instability. No patients had pain at rest, but two patients had mild pain (visual analog scale 1-3) during physical activity. Three patients rated their elbow as normal, one as almost normal, and one as greatly improved. On short-term radiographic follow-up there were no signs of implant loosening. None of the patients needed reoperation.</p><p><strong>Conclusions: </strong>Recurrent PLRI of the elbow associated with an engaging posterior capitellar lesion can be treated successfully by LUCL reconstruction and repair and filling of the capitellar defect with a metal prosthesis. This treatment option has excellent clinical results in the short-medium term. Level of evidence: IV.</p>","PeriodicalId":33981,"journal":{"name":"Clinics in Shoulder and Elbow","volume":"26 3","pages":"287-295"},"PeriodicalIF":1.8000,"publicationDate":"2023-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/f1/50/cise-2022-01424.PMC10497932.pdf","citationCount":"1","resultStr":"{\"title\":\"Prosthetic resurfacing of engaging posterior capitellar defects in recurrent posterolateral rotatory instability of the elbow.\",\"authors\":\"Dani Rotman, Jorge Rojas Lievano, Shawn W O'Driscoll\",\"doi\":\"10.5397/cise.2022.01424\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Posterolateral rotatory instability (PLRI) is a common mechanism of recurrent elbow instability. While the essential lesion is a deficiency in the lateral ulnar collateral ligament (LUCL), there are often associated concomitant bony lesions, such as an Osborne-Cotterill lesions (posterior capitellar fractures) and marginal radial head fractures, that compromise stability. Currently, there is no standard treatment for posterior capitellar deficiency associated with recurrent PLRI.</p><p><strong>Methods: </strong>We conducted a retrospective review of five patients with recurrent PLRI of the elbow associated with a posterior capitellar impaction fracture engaging with the radial head during normal range of motion. The patients were treated surgically with LUCL reconstruction or repair and off-label reconstruction of the capitellar joint surface using a small metal prosthesis designed for metatarsal head resurfacing (HemiCAP toe classic).</p><p><strong>Results: </strong>Five patients (three adolescent males, two adult females) were treated between 2007 and 2018. At a median follow-up of 5 years, all patients had complete relief of their symptomatic instability. No patients had pain at rest, but two patients had mild pain (visual analog scale 1-3) during physical activity. Three patients rated their elbow as normal, one as almost normal, and one as greatly improved. On short-term radiographic follow-up there were no signs of implant loosening. None of the patients needed reoperation.</p><p><strong>Conclusions: </strong>Recurrent PLRI of the elbow associated with an engaging posterior capitellar lesion can be treated successfully by LUCL reconstruction and repair and filling of the capitellar defect with a metal prosthesis. This treatment option has excellent clinical results in the short-medium term. Level of evidence: IV.</p>\",\"PeriodicalId\":33981,\"journal\":{\"name\":\"Clinics in Shoulder and Elbow\",\"volume\":\"26 3\",\"pages\":\"287-295\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2023-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/f1/50/cise-2022-01424.PMC10497932.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinics in Shoulder and Elbow\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5397/cise.2022.01424\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinics in Shoulder and Elbow","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5397/cise.2022.01424","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
Prosthetic resurfacing of engaging posterior capitellar defects in recurrent posterolateral rotatory instability of the elbow.
Background: Posterolateral rotatory instability (PLRI) is a common mechanism of recurrent elbow instability. While the essential lesion is a deficiency in the lateral ulnar collateral ligament (LUCL), there are often associated concomitant bony lesions, such as an Osborne-Cotterill lesions (posterior capitellar fractures) and marginal radial head fractures, that compromise stability. Currently, there is no standard treatment for posterior capitellar deficiency associated with recurrent PLRI.
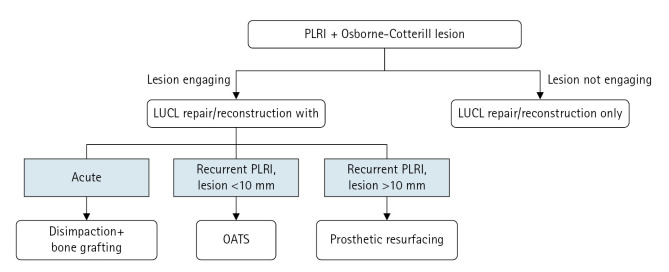
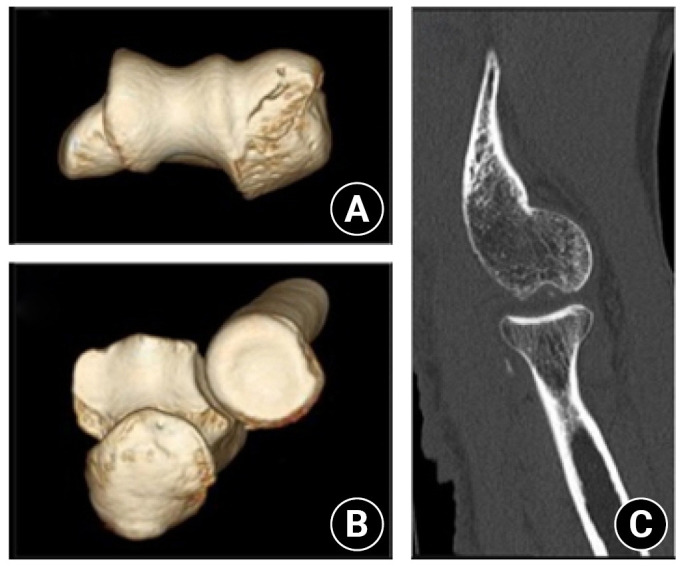
Methods: We conducted a retrospective review of five patients with recurrent PLRI of the elbow associated with a posterior capitellar impaction fracture engaging with the radial head during normal range of motion. The patients were treated surgically with LUCL reconstruction or repair and off-label reconstruction of the capitellar joint surface using a small metal prosthesis designed for metatarsal head resurfacing (HemiCAP toe classic).
Results: Five patients (three adolescent males, two adult females) were treated between 2007 and 2018. At a median follow-up of 5 years, all patients had complete relief of their symptomatic instability. No patients had pain at rest, but two patients had mild pain (visual analog scale 1-3) during physical activity. Three patients rated their elbow as normal, one as almost normal, and one as greatly improved. On short-term radiographic follow-up there were no signs of implant loosening. None of the patients needed reoperation.
Conclusions: Recurrent PLRI of the elbow associated with an engaging posterior capitellar lesion can be treated successfully by LUCL reconstruction and repair and filling of the capitellar defect with a metal prosthesis. This treatment option has excellent clinical results in the short-medium term. Level of evidence: IV.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


