Glenn A Gonzalez, Jingya Miao, Guilherme Porto, James Harrop
{"title":"颈椎后路减压融合手术后双侧膈神经麻痹:术后罕见病例。","authors":"Glenn A Gonzalez, Jingya Miao, Guilherme Porto, James Harrop","doi":"10.1038/s41394-023-00595-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Delayed C5 weakness is a known entity in cervical spine surgery, although with varied clinical presentation and poorly understood mechanism of action. We describe the first case in the literature of a bilateral C5 palsy leading to bilateral phrenic nerve dysfunction following a posterior cervical decompression and fusion.</p><p><strong>Case report: </strong>A 76-year-old male presented with low back pain and was diagnosed as myelopathic. On initial neurological examination, he could not ambulate without assistance and was unsteady on tandem gait. The initial cervical MRI and CT scan showed advanced multilevel degenerative changes of the cervical spine with severe cord compression and myelomalacia. The patient underwent C3-C6 posterior cervical decompression & fusion (PCDF). He awoke with his baseline examination without neurophysiological monitoring changes intraoperatively or C5 root EMG activity. Post-operative MRI of the cervical spine was performed and showed an excellent decompression. The patient was neurologically stable and discharged to a rehabilitation facility. Patient developed a delayed bilateral C5P on postoperative day (POD) 74. Delayed bilateral C5P and phrenic nerve damage was determined to cause this patient's dyspnea. PM&R consult recommended placement of diaphragmatic pacers. However, clinically his respiratory function, as well as motor deficits, have gradually improved.</p><p><strong>Conclusion: </strong>Bilateral diaphragmatic paralysis, a severe complication of cervical spine surgery, may cause respiratory distress and upper limb weakness. C5P, the underlying cause, may arise from various factors. Early detection and management of diaphragmatic weakness with physical therapy and pacers are crucial, emphasizing the need for vigilance by healthcare professionals and surgeons.</p>","PeriodicalId":22079,"journal":{"name":"Spinal Cord Series and Cases","volume":"9 1","pages":"41"},"PeriodicalIF":0.7000,"publicationDate":"2023-08-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10423263/pdf/","citationCount":"0","resultStr":"{\"title\":\"Bilateral phrenic nerve palsy after posterior cervical decompression and fusion surgery: a rare event after surgery.\",\"authors\":\"Glenn A Gonzalez, Jingya Miao, Guilherme Porto, James Harrop\",\"doi\":\"10.1038/s41394-023-00595-1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Delayed C5 weakness is a known entity in cervical spine surgery, although with varied clinical presentation and poorly understood mechanism of action. We describe the first case in the literature of a bilateral C5 palsy leading to bilateral phrenic nerve dysfunction following a posterior cervical decompression and fusion.</p><p><strong>Case report: </strong>A 76-year-old male presented with low back pain and was diagnosed as myelopathic. On initial neurological examination, he could not ambulate without assistance and was unsteady on tandem gait. The initial cervical MRI and CT scan showed advanced multilevel degenerative changes of the cervical spine with severe cord compression and myelomalacia. The patient underwent C3-C6 posterior cervical decompression & fusion (PCDF). He awoke with his baseline examination without neurophysiological monitoring changes intraoperatively or C5 root EMG activity. Post-operative MRI of the cervical spine was performed and showed an excellent decompression. The patient was neurologically stable and discharged to a rehabilitation facility. Patient developed a delayed bilateral C5P on postoperative day (POD) 74. Delayed bilateral C5P and phrenic nerve damage was determined to cause this patient's dyspnea. PM&R consult recommended placement of diaphragmatic pacers. However, clinically his respiratory function, as well as motor deficits, have gradually improved.</p><p><strong>Conclusion: </strong>Bilateral diaphragmatic paralysis, a severe complication of cervical spine surgery, may cause respiratory distress and upper limb weakness. C5P, the underlying cause, may arise from various factors. Early detection and management of diaphragmatic weakness with physical therapy and pacers are crucial, emphasizing the need for vigilance by healthcare professionals and surgeons.</p>\",\"PeriodicalId\":22079,\"journal\":{\"name\":\"Spinal Cord Series and Cases\",\"volume\":\"9 1\",\"pages\":\"41\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2023-08-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10423263/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Spinal Cord Series and Cases\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1038/s41394-023-00595-1\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Spinal Cord Series and Cases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1038/s41394-023-00595-1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Bilateral phrenic nerve palsy after posterior cervical decompression and fusion surgery: a rare event after surgery.
Introduction: Delayed C5 weakness is a known entity in cervical spine surgery, although with varied clinical presentation and poorly understood mechanism of action. We describe the first case in the literature of a bilateral C5 palsy leading to bilateral phrenic nerve dysfunction following a posterior cervical decompression and fusion.
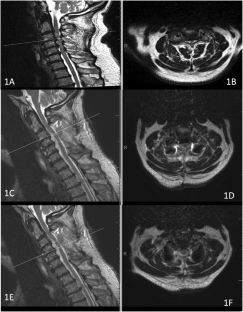
Case report: A 76-year-old male presented with low back pain and was diagnosed as myelopathic. On initial neurological examination, he could not ambulate without assistance and was unsteady on tandem gait. The initial cervical MRI and CT scan showed advanced multilevel degenerative changes of the cervical spine with severe cord compression and myelomalacia. The patient underwent C3-C6 posterior cervical decompression & fusion (PCDF). He awoke with his baseline examination without neurophysiological monitoring changes intraoperatively or C5 root EMG activity. Post-operative MRI of the cervical spine was performed and showed an excellent decompression. The patient was neurologically stable and discharged to a rehabilitation facility. Patient developed a delayed bilateral C5P on postoperative day (POD) 74. Delayed bilateral C5P and phrenic nerve damage was determined to cause this patient's dyspnea. PM&R consult recommended placement of diaphragmatic pacers. However, clinically his respiratory function, as well as motor deficits, have gradually improved.
Conclusion: Bilateral diaphragmatic paralysis, a severe complication of cervical spine surgery, may cause respiratory distress and upper limb weakness. C5P, the underlying cause, may arise from various factors. Early detection and management of diaphragmatic weakness with physical therapy and pacers are crucial, emphasizing the need for vigilance by healthcare professionals and surgeons.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


