Juan Pablo Zicaro, Nicolas Garrido, Ignacio Garcia-Mansilla, Carlos Yacuzzi, Matias Costa-Paz
{"title":"半月板修复后的失败率、恢复运动和磁共振成像:119例患者平均随访7年。","authors":"Juan Pablo Zicaro, Nicolas Garrido, Ignacio Garcia-Mansilla, Carlos Yacuzzi, Matias Costa-Paz","doi":"10.5312/wjo.v14.i8.612","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>One of the most important factors to consider in relation to meniscal repair is the high failure rate reported in the existing literature.</p><p><strong>Aim: </strong>To evaluate failure rates, return to sports (RTS) rate, clinical outcomes and magnetic resonance image (MRI) evaluation after meniscus suture repair for longitudinal tears at a minimum 2-year-follow-up.</p><p><strong>Methods: </strong>We conducted a retrospective review of meniscal repairs between January 2004 and December 2018. All patients treated for longitudinal tears associated or not with an anterior cruciate ligament reconstruction (ACL-R) were included. Meniscal ramp lesions, radial and root tears, associated with multiligament injuries, tibial fracture and meniscal allograft transplants were excluded. Surgical details and failure rate, defined as symptomatic patients who underwent a revision surgery, were analyzed. As isolated bucket handle tears (BHTs) were usually associated with higher failure rates, we compared BHTs and not BHTs associated or not with an ACL-R. Since 2014, the inside-out technique using cannulas and suture needles with 2-0 Tycron began to predominate. In addition, the number of stitches per repair was increased. In view of differences in surgical technique, we compared two different cohorts: before and after 2014. We recorded the RTS according to the level achieved and the time to RTS. Lysholm and IKDC scores were recorded. Patients were studied with x-rays and MRI as standard postoperative control.</p><p><strong>Results: </strong>One hundred and nineteen patients were included with a mean follow up of 7 years (SD: 4.08). Overall failure rate was 20.3% at a mean 20.1 mo. No statistically significant differences were found when comparing failure for medial and lateral meniscal repair (22.7% and 15.3%, <i>P</i> = 0.36), BHTs and not BHTs (26% and 17.6%, <i>P</i> = 0.27), isolated or associated with an ACL-R (22.9% and 18%, <i>P</i> = 0.47), or when comparing only BHTs associated with an ACL-R (23% and 27.7%, <i>P</i> = 0.9) or not. When comparing cohorts before and after 2014, we found a significant decrease in the overall failure rate from 26% to 11% (<i>P</i> < 0.03). Isolated lesions presented a decrease from 28% to 6.6% (<i>P</i> = 0.02), BHTs from 34% to 8% (<i>P</i> = 0.09) and those associated with an ACL-R from 25% to 10% (<i>P</i> = 0.09). Mean RTS time was 6.5 mo in isolated lesions and 8.64 mo when associated with an ACL-R. Overall, 56% of patients returned to the same sport activity level. Mean pre and postoperative Lysholm scores were 64 and 85 (<i>P</i> = 0.02), and IKDC 58 and 70 (<i>P</i> = 0.03). Out of 84 asymptomatic patients evaluated with MRI, 39% were classified as \"not healed\" and 61% as \"healed\".</p><p><strong>Conclusion: </strong>Even though the overall failure rate of our series was 20.3%, we found a statistically significant decrease from 26% to 11%, not only for isolated lesions, but also for BHT's and those associated with an ACL-R when comparing our series in two different cohorts, most probably due to improvements in surgical technique.</p>","PeriodicalId":47843,"journal":{"name":"World Journal of Orthopedics","volume":"14 8","pages":"612-620"},"PeriodicalIF":2.0000,"publicationDate":"2023-08-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d1/85/WJO-14-612.PMC10473908.pdf","citationCount":"0","resultStr":"{\"title\":\"Failure rate, return-to-sports and magnetic resonance imaging after meniscal repair: 119 patients with 7 years mean follow up.\",\"authors\":\"Juan Pablo Zicaro, Nicolas Garrido, Ignacio Garcia-Mansilla, Carlos Yacuzzi, Matias Costa-Paz\",\"doi\":\"10.5312/wjo.v14.i8.612\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>One of the most important factors to consider in relation to meniscal repair is the high failure rate reported in the existing literature.</p><p><strong>Aim: </strong>To evaluate failure rates, return to sports (RTS) rate, clinical outcomes and magnetic resonance image (MRI) evaluation after meniscus suture repair for longitudinal tears at a minimum 2-year-follow-up.</p><p><strong>Methods: </strong>We conducted a retrospective review of meniscal repairs between January 2004 and December 2018. All patients treated for longitudinal tears associated or not with an anterior cruciate ligament reconstruction (ACL-R) were included. Meniscal ramp lesions, radial and root tears, associated with multiligament injuries, tibial fracture and meniscal allograft transplants were excluded. Surgical details and failure rate, defined as symptomatic patients who underwent a revision surgery, were analyzed. As isolated bucket handle tears (BHTs) were usually associated with higher failure rates, we compared BHTs and not BHTs associated or not with an ACL-R. Since 2014, the inside-out technique using cannulas and suture needles with 2-0 Tycron began to predominate. In addition, the number of stitches per repair was increased. In view of differences in surgical technique, we compared two different cohorts: before and after 2014. We recorded the RTS according to the level achieved and the time to RTS. Lysholm and IKDC scores were recorded. Patients were studied with x-rays and MRI as standard postoperative control.</p><p><strong>Results: </strong>One hundred and nineteen patients were included with a mean follow up of 7 years (SD: 4.08). Overall failure rate was 20.3% at a mean 20.1 mo. No statistically significant differences were found when comparing failure for medial and lateral meniscal repair (22.7% and 15.3%, <i>P</i> = 0.36), BHTs and not BHTs (26% and 17.6%, <i>P</i> = 0.27), isolated or associated with an ACL-R (22.9% and 18%, <i>P</i> = 0.47), or when comparing only BHTs associated with an ACL-R (23% and 27.7%, <i>P</i> = 0.9) or not. When comparing cohorts before and after 2014, we found a significant decrease in the overall failure rate from 26% to 11% (<i>P</i> < 0.03). Isolated lesions presented a decrease from 28% to 6.6% (<i>P</i> = 0.02), BHTs from 34% to 8% (<i>P</i> = 0.09) and those associated with an ACL-R from 25% to 10% (<i>P</i> = 0.09). Mean RTS time was 6.5 mo in isolated lesions and 8.64 mo when associated with an ACL-R. Overall, 56% of patients returned to the same sport activity level. Mean pre and postoperative Lysholm scores were 64 and 85 (<i>P</i> = 0.02), and IKDC 58 and 70 (<i>P</i> = 0.03). Out of 84 asymptomatic patients evaluated with MRI, 39% were classified as \\\"not healed\\\" and 61% as \\\"healed\\\".</p><p><strong>Conclusion: </strong>Even though the overall failure rate of our series was 20.3%, we found a statistically significant decrease from 26% to 11%, not only for isolated lesions, but also for BHT's and those associated with an ACL-R when comparing our series in two different cohorts, most probably due to improvements in surgical technique.</p>\",\"PeriodicalId\":47843,\"journal\":{\"name\":\"World Journal of Orthopedics\",\"volume\":\"14 8\",\"pages\":\"612-620\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2023-08-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d1/85/WJO-14-612.PMC10473908.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World Journal of Orthopedics\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5312/wjo.v14.i8.612\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Orthopedics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5312/wjo.v14.i8.612","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
Failure rate, return-to-sports and magnetic resonance imaging after meniscal repair: 119 patients with 7 years mean follow up.
Background: One of the most important factors to consider in relation to meniscal repair is the high failure rate reported in the existing literature.
Aim: To evaluate failure rates, return to sports (RTS) rate, clinical outcomes and magnetic resonance image (MRI) evaluation after meniscus suture repair for longitudinal tears at a minimum 2-year-follow-up.
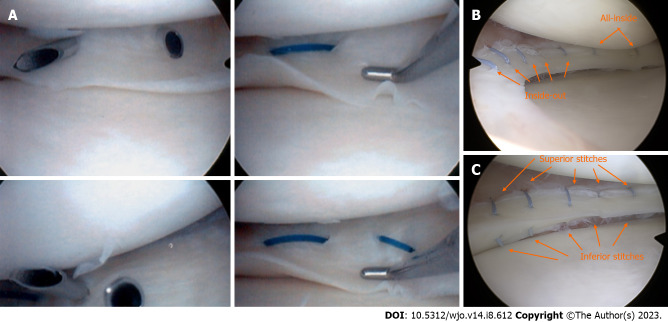
Methods: We conducted a retrospective review of meniscal repairs between January 2004 and December 2018. All patients treated for longitudinal tears associated or not with an anterior cruciate ligament reconstruction (ACL-R) were included. Meniscal ramp lesions, radial and root tears, associated with multiligament injuries, tibial fracture and meniscal allograft transplants were excluded. Surgical details and failure rate, defined as symptomatic patients who underwent a revision surgery, were analyzed. As isolated bucket handle tears (BHTs) were usually associated with higher failure rates, we compared BHTs and not BHTs associated or not with an ACL-R. Since 2014, the inside-out technique using cannulas and suture needles with 2-0 Tycron began to predominate. In addition, the number of stitches per repair was increased. In view of differences in surgical technique, we compared two different cohorts: before and after 2014. We recorded the RTS according to the level achieved and the time to RTS. Lysholm and IKDC scores were recorded. Patients were studied with x-rays and MRI as standard postoperative control.
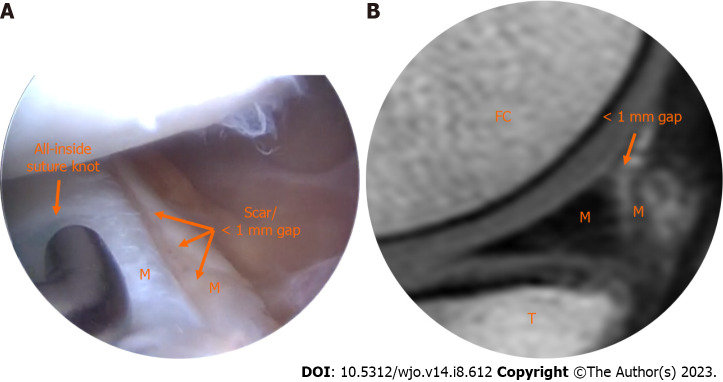
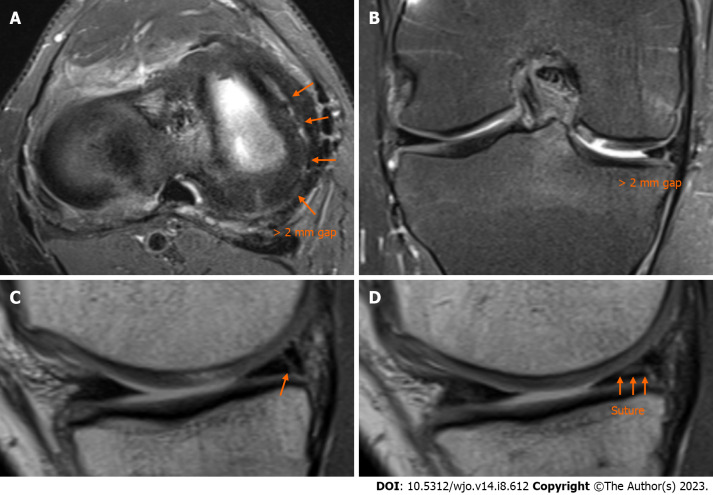
Results: One hundred and nineteen patients were included with a mean follow up of 7 years (SD: 4.08). Overall failure rate was 20.3% at a mean 20.1 mo. No statistically significant differences were found when comparing failure for medial and lateral meniscal repair (22.7% and 15.3%, P = 0.36), BHTs and not BHTs (26% and 17.6%, P = 0.27), isolated or associated with an ACL-R (22.9% and 18%, P = 0.47), or when comparing only BHTs associated with an ACL-R (23% and 27.7%, P = 0.9) or not. When comparing cohorts before and after 2014, we found a significant decrease in the overall failure rate from 26% to 11% (P < 0.03). Isolated lesions presented a decrease from 28% to 6.6% (P = 0.02), BHTs from 34% to 8% (P = 0.09) and those associated with an ACL-R from 25% to 10% (P = 0.09). Mean RTS time was 6.5 mo in isolated lesions and 8.64 mo when associated with an ACL-R. Overall, 56% of patients returned to the same sport activity level. Mean pre and postoperative Lysholm scores were 64 and 85 (P = 0.02), and IKDC 58 and 70 (P = 0.03). Out of 84 asymptomatic patients evaluated with MRI, 39% were classified as "not healed" and 61% as "healed".
Conclusion: Even though the overall failure rate of our series was 20.3%, we found a statistically significant decrease from 26% to 11%, not only for isolated lesions, but also for BHT's and those associated with an ACL-R when comparing our series in two different cohorts, most probably due to improvements in surgical technique.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


