{"title":"自身免疫性边缘脑炎合并非小细胞肺癌轻脑膜转移:对奥希替尼、免疫球蛋白、利妥昔单抗和托珠单抗的治疗反应","authors":"Seolah Lee, Seon-Jae Ahn, Han Sang Lee, Kon Chu","doi":"10.47936/encephalitis.2022.00122","DOIUrl":null,"url":null,"abstract":"<p><p>When a patient with encephalopathy has an organic brain lesion, his symptom is easily and often mistakenly attributed to that brain lesion. However, a combination of different conditions is also possible. We present a case of autoimmune limbic encephalitis combined with leptomeningeal carcinomatosis. A 57-year-old female patient was transferred to our institute with a 1-month history of seizure and aggressive behavior. Subacute onset of psychosis with multifocal T2 high signal lesions suggested autoimmune encephalitis, and high-dose steroid pulse and immunoglobulin therapy were started. However, a cerebrospinal fluid study revealed metastatic adenocarcinoma of non-small cell lung cancer, of which she was in complete remission state. Osimertinib, a third-generation epidermal growth factor receptor tyrosine kinase inhibitor, was started targeting leptomeningeal metastases while maintaining immunotherapy of rituximab and tocilizumab. Her neurological symptoms showed improvement in response to immunotherapy which lasted approximately 1 month and then deteriorated again. We concluded that her symptoms were more attributable to autoimmune encephalitis than leptomeningeal carcinomatosis, and discontinued osimertinib.</p>","PeriodicalId":72904,"journal":{"name":"Encephalitis (Seoul, Korea)","volume":"3 1","pages":"34-38"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1b/00/encephalitis-2022-00122.PMC10295819.pdf","citationCount":"0","resultStr":"{\"title\":\"Autoimmune limbic encephalitis combined with leptomeningeal metastases of non-small cell lung cancer: treatment response to osimertinib, immunoglobulin, rituximab, and tocilizumab.\",\"authors\":\"Seolah Lee, Seon-Jae Ahn, Han Sang Lee, Kon Chu\",\"doi\":\"10.47936/encephalitis.2022.00122\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>When a patient with encephalopathy has an organic brain lesion, his symptom is easily and often mistakenly attributed to that brain lesion. However, a combination of different conditions is also possible. We present a case of autoimmune limbic encephalitis combined with leptomeningeal carcinomatosis. A 57-year-old female patient was transferred to our institute with a 1-month history of seizure and aggressive behavior. Subacute onset of psychosis with multifocal T2 high signal lesions suggested autoimmune encephalitis, and high-dose steroid pulse and immunoglobulin therapy were started. However, a cerebrospinal fluid study revealed metastatic adenocarcinoma of non-small cell lung cancer, of which she was in complete remission state. Osimertinib, a third-generation epidermal growth factor receptor tyrosine kinase inhibitor, was started targeting leptomeningeal metastases while maintaining immunotherapy of rituximab and tocilizumab. Her neurological symptoms showed improvement in response to immunotherapy which lasted approximately 1 month and then deteriorated again. We concluded that her symptoms were more attributable to autoimmune encephalitis than leptomeningeal carcinomatosis, and discontinued osimertinib.</p>\",\"PeriodicalId\":72904,\"journal\":{\"name\":\"Encephalitis (Seoul, Korea)\",\"volume\":\"3 1\",\"pages\":\"34-38\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1b/00/encephalitis-2022-00122.PMC10295819.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Encephalitis (Seoul, Korea)\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.47936/encephalitis.2022.00122\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Encephalitis (Seoul, Korea)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.47936/encephalitis.2022.00122","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Autoimmune limbic encephalitis combined with leptomeningeal metastases of non-small cell lung cancer: treatment response to osimertinib, immunoglobulin, rituximab, and tocilizumab.
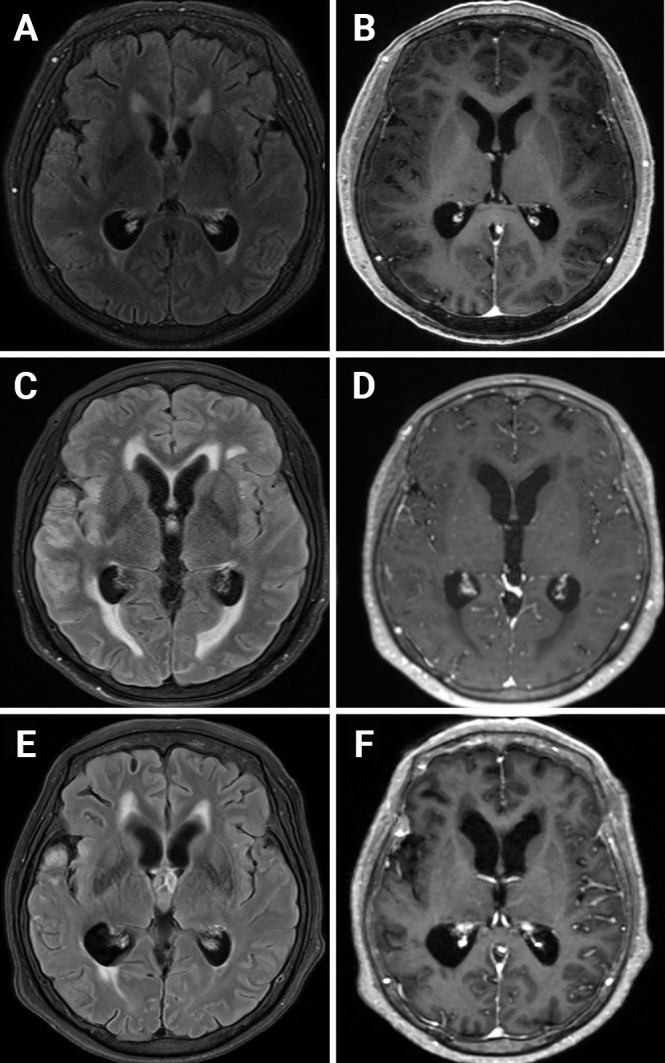
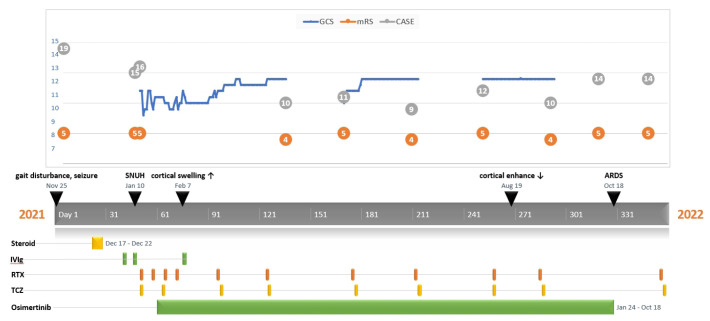
When a patient with encephalopathy has an organic brain lesion, his symptom is easily and often mistakenly attributed to that brain lesion. However, a combination of different conditions is also possible. We present a case of autoimmune limbic encephalitis combined with leptomeningeal carcinomatosis. A 57-year-old female patient was transferred to our institute with a 1-month history of seizure and aggressive behavior. Subacute onset of psychosis with multifocal T2 high signal lesions suggested autoimmune encephalitis, and high-dose steroid pulse and immunoglobulin therapy were started. However, a cerebrospinal fluid study revealed metastatic adenocarcinoma of non-small cell lung cancer, of which she was in complete remission state. Osimertinib, a third-generation epidermal growth factor receptor tyrosine kinase inhibitor, was started targeting leptomeningeal metastases while maintaining immunotherapy of rituximab and tocilizumab. Her neurological symptoms showed improvement in response to immunotherapy which lasted approximately 1 month and then deteriorated again. We concluded that her symptoms were more attributable to autoimmune encephalitis than leptomeningeal carcinomatosis, and discontinued osimertinib.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


