{"title":"利培酮过量后造影剂引起的肾上腺素抵抗性过敏性休克1例报告。","authors":"Takafumi Nakano, Yoshihiko Nakamura, Keisuke Sato, Yoshito Izutani, Hiroto Iyota, Misaki Aoyagi, Taisuke Kitamura, Toshinobu Hayashi, Koichi Matsuo, Kenichi Mishima, Hidetoshi Kamimura, Hiroyasu Ishikura, Takashi Egawa","doi":"10.1186/s40780-023-00292-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In Japan, the use of risperidone in combination with adrenaline is contraindicated, except in cases of anaphylaxis. Therefore, there is limited clinical evidence regarding the interaction of these two drugs. Here, we report the clinical course of a case of adrenaline-resistant anaphylactic shock induced by a contrast medium injection after a risperidone overdose.</p><p><strong>Case presentation: </strong>A man in his 30s was transported to our hospital after attempting suicide by taking 10 mg of risperidone and jumping from a height of 10 m. To determine the location and severity of his injuries, he was injected with an iodinated contrast medium, after which he developed generalized erythema and hypotension and was diagnosed with anaphylactic shock. A 0.5 mg dose of adrenaline was administered with no improvement, followed by another 0.5 mg dose that did not change his blood pressure. After infusion of a sodium bicarbonate solution (8.4%), administration of fresh frozen plasma, and additional administration of adrenaline (0.6-1.2 µg/min), his blood pressure improved, and he recovered from the anaphylactic shock.</p><p><strong>Conclusions: </strong>This was a rare case of a risperidone overdose followed by adrenaline-resistant anaphylactic shock. The resistance is likely associated with the high blood concentration of risperidone. Our findings indicate that the potential for decreased adrenergic responsiveness should be considered in patients undergoing risperidone treatment in the event of anaphylactic shock.</p>","PeriodicalId":16730,"journal":{"name":"Journal of Pharmaceutical Health Care and Sciences","volume":null,"pages":null},"PeriodicalIF":1.2000,"publicationDate":"2023-07-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10337192/pdf/","citationCount":"1","resultStr":"{\"title\":\"Adrenaline-resistant anaphylactic shock caused by contrast medium in a patient after risperidone overdose: a case report.\",\"authors\":\"Takafumi Nakano, Yoshihiko Nakamura, Keisuke Sato, Yoshito Izutani, Hiroto Iyota, Misaki Aoyagi, Taisuke Kitamura, Toshinobu Hayashi, Koichi Matsuo, Kenichi Mishima, Hidetoshi Kamimura, Hiroyasu Ishikura, Takashi Egawa\",\"doi\":\"10.1186/s40780-023-00292-z\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>In Japan, the use of risperidone in combination with adrenaline is contraindicated, except in cases of anaphylaxis. Therefore, there is limited clinical evidence regarding the interaction of these two drugs. Here, we report the clinical course of a case of adrenaline-resistant anaphylactic shock induced by a contrast medium injection after a risperidone overdose.</p><p><strong>Case presentation: </strong>A man in his 30s was transported to our hospital after attempting suicide by taking 10 mg of risperidone and jumping from a height of 10 m. To determine the location and severity of his injuries, he was injected with an iodinated contrast medium, after which he developed generalized erythema and hypotension and was diagnosed with anaphylactic shock. A 0.5 mg dose of adrenaline was administered with no improvement, followed by another 0.5 mg dose that did not change his blood pressure. After infusion of a sodium bicarbonate solution (8.4%), administration of fresh frozen plasma, and additional administration of adrenaline (0.6-1.2 µg/min), his blood pressure improved, and he recovered from the anaphylactic shock.</p><p><strong>Conclusions: </strong>This was a rare case of a risperidone overdose followed by adrenaline-resistant anaphylactic shock. The resistance is likely associated with the high blood concentration of risperidone. Our findings indicate that the potential for decreased adrenergic responsiveness should be considered in patients undergoing risperidone treatment in the event of anaphylactic shock.</p>\",\"PeriodicalId\":16730,\"journal\":{\"name\":\"Journal of Pharmaceutical Health Care and Sciences\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2023-07-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10337192/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Pharmaceutical Health Care and Sciences\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s40780-023-00292-z\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Pharmaceutical Health Care and Sciences","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40780-023-00292-z","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
Adrenaline-resistant anaphylactic shock caused by contrast medium in a patient after risperidone overdose: a case report.
Background: In Japan, the use of risperidone in combination with adrenaline is contraindicated, except in cases of anaphylaxis. Therefore, there is limited clinical evidence regarding the interaction of these two drugs. Here, we report the clinical course of a case of adrenaline-resistant anaphylactic shock induced by a contrast medium injection after a risperidone overdose.
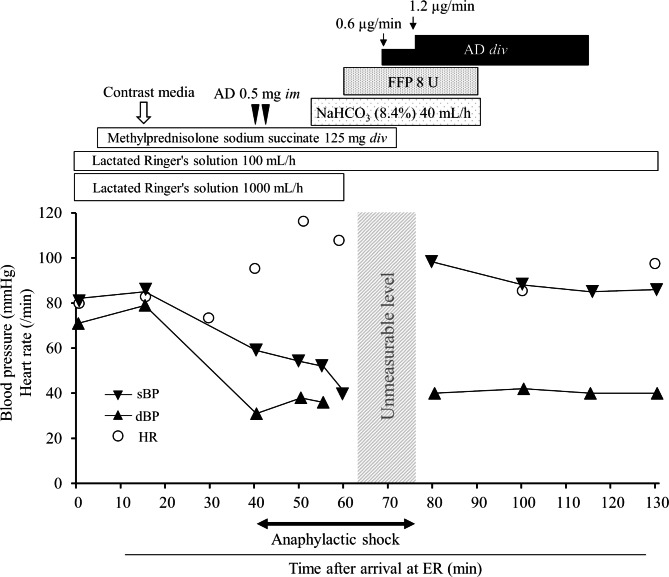
Case presentation: A man in his 30s was transported to our hospital after attempting suicide by taking 10 mg of risperidone and jumping from a height of 10 m. To determine the location and severity of his injuries, he was injected with an iodinated contrast medium, after which he developed generalized erythema and hypotension and was diagnosed with anaphylactic shock. A 0.5 mg dose of adrenaline was administered with no improvement, followed by another 0.5 mg dose that did not change his blood pressure. After infusion of a sodium bicarbonate solution (8.4%), administration of fresh frozen plasma, and additional administration of adrenaline (0.6-1.2 µg/min), his blood pressure improved, and he recovered from the anaphylactic shock.
Conclusions: This was a rare case of a risperidone overdose followed by adrenaline-resistant anaphylactic shock. The resistance is likely associated with the high blood concentration of risperidone. Our findings indicate that the potential for decreased adrenergic responsiveness should be considered in patients undergoing risperidone treatment in the event of anaphylactic shock.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


