Youngbo Shim, Jungook Kim, Hye Seon Kim, Jiwoong Oh, Seungioo Lee, Eun Jin Ha
{"title":"急性脑损伤患者的颅内压监测:何时,如何监测,应该监测什么。","authors":"Youngbo Shim, Jungook Kim, Hye Seon Kim, Jiwoong Oh, Seungioo Lee, Eun Jin Ha","doi":"10.13004/kjnt.2023.19.e32","DOIUrl":null,"url":null,"abstract":"<p><p>While there is no level I recommendation for intracranial pressure (ICP) monitoring, it is typically indicated for patients with severe traumatic brain injury (TBI) with a Glasgow Coma Scale (GCS) score of 3-8 (class II). Even for moderate TBI patients with GCS 9-12, ICP monitoring should be considered for risk of increased ICP. The impact of ICP monitoring on patient outcomes is still not well-established, but recent studies reported a reduction of early mortality (class III) in TBI patients. There is no standard protocol for the application of ICP monitoring. In cases where cerebrospinal fluid drainage is required, an external ventricular drain is commonly used. In other cases, parenchymal ICP monitoring devices are generally employed. Subdural or non-invasive forms are not suitable for ICP monitoring. The mean value of ICP is the parameter recommended for observation in many guidelines. In TBI, values above 22 mmHg are associated with increased mortality. However, recent studies proposed various parameters including cumulative time with ICP above 20 mmHg (pressure-time dose), pressure reactivity index, ICP waveform characteristics (pulse amplitude of ICP, mean ICP wave amplitude), and the compensatory reserve of the brain (reserve-amplitude-pressure), which are useful in predicting patient outcomes and guiding treatment. Further research is required for validation of these parameters compared to simple ICP monitoring.</p>","PeriodicalId":36879,"journal":{"name":"Korean Journal of Neurotrauma","volume":"19 2","pages":"149-161"},"PeriodicalIF":0.0000,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/03/e6/kjn-19-149.PMC10329885.pdf","citationCount":"0","resultStr":"{\"title\":\"Intracranial Pressure Monitoring for Acute Brain Injured Patients: When, How, What Should We Monitor.\",\"authors\":\"Youngbo Shim, Jungook Kim, Hye Seon Kim, Jiwoong Oh, Seungioo Lee, Eun Jin Ha\",\"doi\":\"10.13004/kjnt.2023.19.e32\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>While there is no level I recommendation for intracranial pressure (ICP) monitoring, it is typically indicated for patients with severe traumatic brain injury (TBI) with a Glasgow Coma Scale (GCS) score of 3-8 (class II). Even for moderate TBI patients with GCS 9-12, ICP monitoring should be considered for risk of increased ICP. The impact of ICP monitoring on patient outcomes is still not well-established, but recent studies reported a reduction of early mortality (class III) in TBI patients. There is no standard protocol for the application of ICP monitoring. In cases where cerebrospinal fluid drainage is required, an external ventricular drain is commonly used. In other cases, parenchymal ICP monitoring devices are generally employed. Subdural or non-invasive forms are not suitable for ICP monitoring. The mean value of ICP is the parameter recommended for observation in many guidelines. In TBI, values above 22 mmHg are associated with increased mortality. However, recent studies proposed various parameters including cumulative time with ICP above 20 mmHg (pressure-time dose), pressure reactivity index, ICP waveform characteristics (pulse amplitude of ICP, mean ICP wave amplitude), and the compensatory reserve of the brain (reserve-amplitude-pressure), which are useful in predicting patient outcomes and guiding treatment. Further research is required for validation of these parameters compared to simple ICP monitoring.</p>\",\"PeriodicalId\":36879,\"journal\":{\"name\":\"Korean Journal of Neurotrauma\",\"volume\":\"19 2\",\"pages\":\"149-161\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/03/e6/kjn-19-149.PMC10329885.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Korean Journal of Neurotrauma\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.13004/kjnt.2023.19.e32\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Korean Journal of Neurotrauma","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.13004/kjnt.2023.19.e32","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
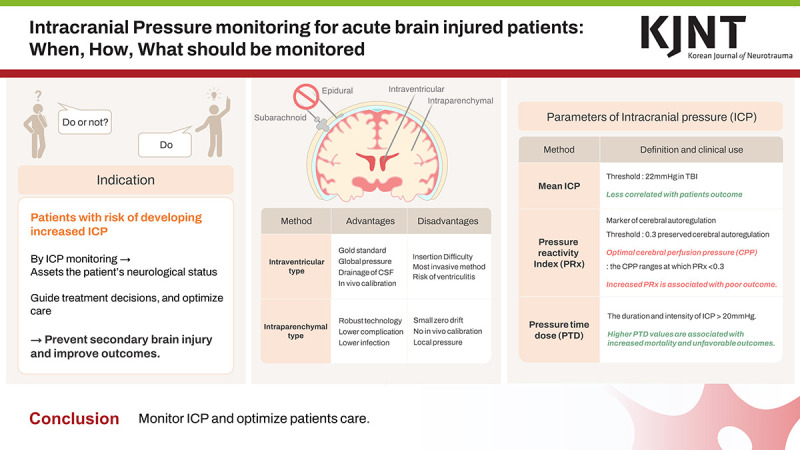
Intracranial Pressure Monitoring for Acute Brain Injured Patients: When, How, What Should We Monitor.
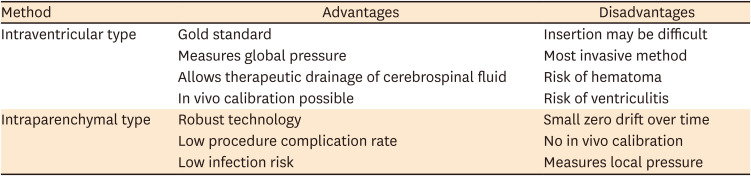
While there is no level I recommendation for intracranial pressure (ICP) monitoring, it is typically indicated for patients with severe traumatic brain injury (TBI) with a Glasgow Coma Scale (GCS) score of 3-8 (class II). Even for moderate TBI patients with GCS 9-12, ICP monitoring should be considered for risk of increased ICP. The impact of ICP monitoring on patient outcomes is still not well-established, but recent studies reported a reduction of early mortality (class III) in TBI patients. There is no standard protocol for the application of ICP monitoring. In cases where cerebrospinal fluid drainage is required, an external ventricular drain is commonly used. In other cases, parenchymal ICP monitoring devices are generally employed. Subdural or non-invasive forms are not suitable for ICP monitoring. The mean value of ICP is the parameter recommended for observation in many guidelines. In TBI, values above 22 mmHg are associated with increased mortality. However, recent studies proposed various parameters including cumulative time with ICP above 20 mmHg (pressure-time dose), pressure reactivity index, ICP waveform characteristics (pulse amplitude of ICP, mean ICP wave amplitude), and the compensatory reserve of the brain (reserve-amplitude-pressure), which are useful in predicting patient outcomes and guiding treatment. Further research is required for validation of these parameters compared to simple ICP monitoring.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


