{"title":"出血性膀胱炎:快速和精明的临床和手术决策,以改善患者的预后。","authors":"Francis A Jefferson, Brian J Linder","doi":"10.2147/RRU.S320684","DOIUrl":null,"url":null,"abstract":"<p><p>Hemorrhagic cystitis (HC) can be one of the most challenging clinical scenarios for urologists to manage. It most commonly occurs as a toxicity of pelvic radiation therapy or in patients treated with the oxazaphosphorine class of chemotherapy. Successful management of HC necessitates a stepwise approach with a thorough understanding of the various treatment options. Once ensuring hemodynamic stability, conservative management includes establishing bladder drainage, manual clot evacuation, and continuous bladder irrigation through a large-bore urethral catheter. If gross hematuria persists, operative cystoscopy with bladder clot evacuation is often required. There are multiple intravesical options for treating HC, including alum, aminocaproic acid, prostaglandins, silver nitrate, and formalin. Formalin is an intravesical option that has caustic effects on the bladder mucosa and is most often reserved as a last-line intravesical treatment. Non-intravesical management tools include hyperbaric oxygen therapy and oral pentosan polysulfate. If needed, nephrostomy tube placement or superselective angioembolization of the anterior division of the internal iliac artery can be performed. Finally, cystectomy with urinary diversion is a definitive, albeit invasive, treatment option for refractory HC. While there is no standardized algorithm, treatment modalities typically progress from less to more invasive. Clinical judgement and shared decision-making with the patient are required when choosing therapies for managing HC, as success rates are variable and some treatments may have significant or irreversible effects.</p>","PeriodicalId":21008,"journal":{"name":"Research and Reports in Urology","volume":null,"pages":null},"PeriodicalIF":2.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/f4/00/rru-15-291.PMC10317550.pdf","citationCount":"0","resultStr":"{\"title\":\"Hemorrhagic Cystitis: Making Rapid and Shrewd Clinical and Surgical Decisions for Improving Patient Outcomes.\",\"authors\":\"Francis A Jefferson, Brian J Linder\",\"doi\":\"10.2147/RRU.S320684\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Hemorrhagic cystitis (HC) can be one of the most challenging clinical scenarios for urologists to manage. It most commonly occurs as a toxicity of pelvic radiation therapy or in patients treated with the oxazaphosphorine class of chemotherapy. Successful management of HC necessitates a stepwise approach with a thorough understanding of the various treatment options. Once ensuring hemodynamic stability, conservative management includes establishing bladder drainage, manual clot evacuation, and continuous bladder irrigation through a large-bore urethral catheter. If gross hematuria persists, operative cystoscopy with bladder clot evacuation is often required. There are multiple intravesical options for treating HC, including alum, aminocaproic acid, prostaglandins, silver nitrate, and formalin. Formalin is an intravesical option that has caustic effects on the bladder mucosa and is most often reserved as a last-line intravesical treatment. Non-intravesical management tools include hyperbaric oxygen therapy and oral pentosan polysulfate. If needed, nephrostomy tube placement or superselective angioembolization of the anterior division of the internal iliac artery can be performed. Finally, cystectomy with urinary diversion is a definitive, albeit invasive, treatment option for refractory HC. While there is no standardized algorithm, treatment modalities typically progress from less to more invasive. Clinical judgement and shared decision-making with the patient are required when choosing therapies for managing HC, as success rates are variable and some treatments may have significant or irreversible effects.</p>\",\"PeriodicalId\":21008,\"journal\":{\"name\":\"Research and Reports in Urology\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/f4/00/rru-15-291.PMC10317550.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Research and Reports in Urology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/RRU.S320684\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Research and Reports in Urology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/RRU.S320684","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
Hemorrhagic Cystitis: Making Rapid and Shrewd Clinical and Surgical Decisions for Improving Patient Outcomes.
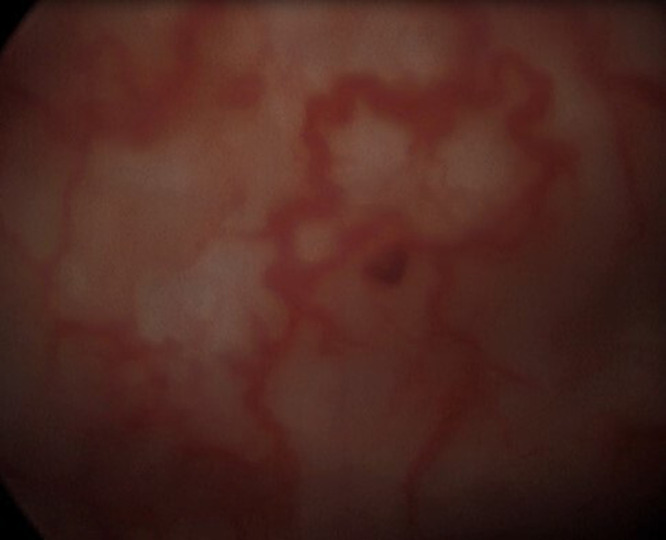
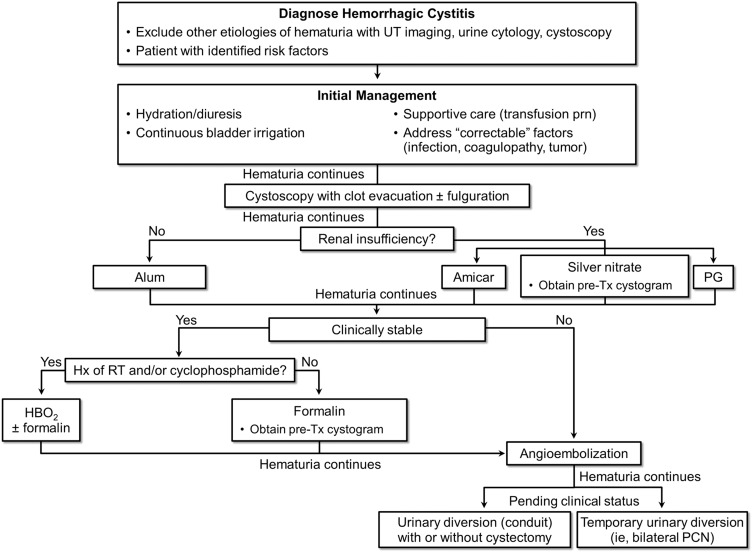
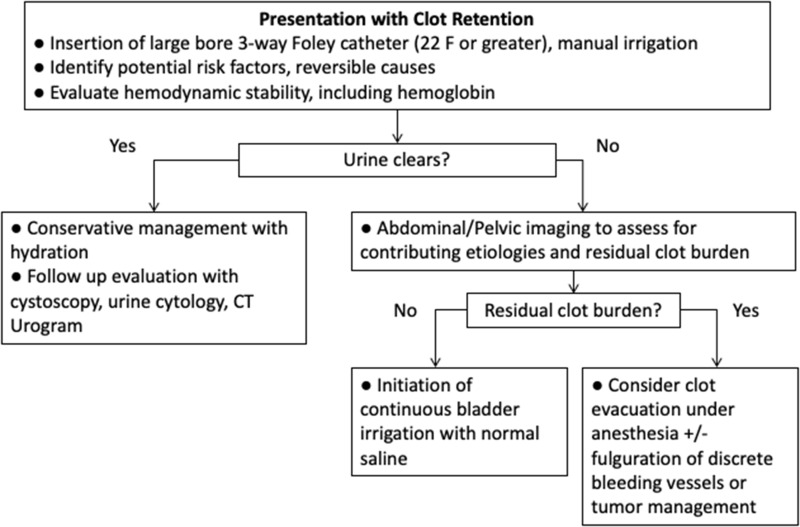
Hemorrhagic cystitis (HC) can be one of the most challenging clinical scenarios for urologists to manage. It most commonly occurs as a toxicity of pelvic radiation therapy or in patients treated with the oxazaphosphorine class of chemotherapy. Successful management of HC necessitates a stepwise approach with a thorough understanding of the various treatment options. Once ensuring hemodynamic stability, conservative management includes establishing bladder drainage, manual clot evacuation, and continuous bladder irrigation through a large-bore urethral catheter. If gross hematuria persists, operative cystoscopy with bladder clot evacuation is often required. There are multiple intravesical options for treating HC, including alum, aminocaproic acid, prostaglandins, silver nitrate, and formalin. Formalin is an intravesical option that has caustic effects on the bladder mucosa and is most often reserved as a last-line intravesical treatment. Non-intravesical management tools include hyperbaric oxygen therapy and oral pentosan polysulfate. If needed, nephrostomy tube placement or superselective angioembolization of the anterior division of the internal iliac artery can be performed. Finally, cystectomy with urinary diversion is a definitive, albeit invasive, treatment option for refractory HC. While there is no standardized algorithm, treatment modalities typically progress from less to more invasive. Clinical judgement and shared decision-making with the patient are required when choosing therapies for managing HC, as success rates are variable and some treatments may have significant or irreversible effects.
期刊介绍:
Research and Reports in Urology is an international, peer-reviewed, open access, online journal. Publishing original research, reports, editorials, reviews and commentaries on all aspects of adult and pediatric urology in the clinic and laboratory including the following topics: Pathology, pathophysiology of urological disease Investigation and treatment of urological disease Pharmacology of drugs used for the treatment of urological disease Although the main focus of the journal is to publish research and clinical results in humans; preclinical, animal and in vitro studies will be published where they will shed light on disease processes and potential new therapies. Issues of patient safety and quality of care will also be considered.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


