{"title":"含有t(11;14)和1q扩增的IgE浆细胞白血病。","authors":"Wataru Nakahara, Takahito Ogawa, Hitomi Matsunaga, Yuki Iwasa, Momoka Horita, Mako Ikeda, Mizuki Asako, Sadaharu Iio, Yuki Iwama, Kazumasa Oka, Shuji Ueda","doi":"10.1155/2023/4747989","DOIUrl":null,"url":null,"abstract":"<p><p>IgE plasma cell neoplasm is the rarest subtype of plasma cell neoplasms and is known for its poor prognosis and high incidence of t(11;14). However, t(11;14) has been classified as a standard-risk rather than high-risk cytogenetic abnormality in multiple myeloma. We have been unable to explain the discrepancy that the hallmark of IgE plasma cell neoplasm with a poor prognosis is a standard-risk cytogenetic abnormality. Here, we report a case of IgE primary plasma cell leukemia with extramedullary lesions of the liver, stomach, and lymph nodes. Plasma cell infiltration was pathologically confirmed in each organ. Cytogenetic analysis of plasma cells revealed t(11;14) and amplification of 1q21. Chemotherapy, with immunomodulatory imide drugs, proteasome inhibitors, and CD38 antibodies, was unsuccessful. In IgE plasma cell neoplasm, coexistence of other cytogenetic abnormalities with t(11;14) may be important. Investigating the presence of cytogenetic abnormalities coexisting with t(11;14) is not only useful for evaluating prognosis but also important for understanding the pathogenesis of the disease. Recently, venetoclax, an oral BCL2 inhibitor, has demonstrated promising efficacy in plasma cell neoplasm patients harboring t(11;14). Development of an effective venetoclax-based regimen for treating aggressive IgE plasma cell neoplasm with t(11;14) is expected.</p>","PeriodicalId":46307,"journal":{"name":"Case Reports in Hematology","volume":"2023 ","pages":"4747989"},"PeriodicalIF":0.7000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10319461/pdf/","citationCount":"1","resultStr":"{\"title\":\"IgE Plasma Cell Leukemia Harboring t(11;14) and 1q Amplification.\",\"authors\":\"Wataru Nakahara, Takahito Ogawa, Hitomi Matsunaga, Yuki Iwasa, Momoka Horita, Mako Ikeda, Mizuki Asako, Sadaharu Iio, Yuki Iwama, Kazumasa Oka, Shuji Ueda\",\"doi\":\"10.1155/2023/4747989\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>IgE plasma cell neoplasm is the rarest subtype of plasma cell neoplasms and is known for its poor prognosis and high incidence of t(11;14). However, t(11;14) has been classified as a standard-risk rather than high-risk cytogenetic abnormality in multiple myeloma. We have been unable to explain the discrepancy that the hallmark of IgE plasma cell neoplasm with a poor prognosis is a standard-risk cytogenetic abnormality. Here, we report a case of IgE primary plasma cell leukemia with extramedullary lesions of the liver, stomach, and lymph nodes. Plasma cell infiltration was pathologically confirmed in each organ. Cytogenetic analysis of plasma cells revealed t(11;14) and amplification of 1q21. Chemotherapy, with immunomodulatory imide drugs, proteasome inhibitors, and CD38 antibodies, was unsuccessful. In IgE plasma cell neoplasm, coexistence of other cytogenetic abnormalities with t(11;14) may be important. Investigating the presence of cytogenetic abnormalities coexisting with t(11;14) is not only useful for evaluating prognosis but also important for understanding the pathogenesis of the disease. Recently, venetoclax, an oral BCL2 inhibitor, has demonstrated promising efficacy in plasma cell neoplasm patients harboring t(11;14). Development of an effective venetoclax-based regimen for treating aggressive IgE plasma cell neoplasm with t(11;14) is expected.</p>\",\"PeriodicalId\":46307,\"journal\":{\"name\":\"Case Reports in Hematology\",\"volume\":\"2023 \",\"pages\":\"4747989\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10319461/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Hematology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2023/4747989\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Hematology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2023/4747989","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"HEMATOLOGY","Score":null,"Total":0}
IgE Plasma Cell Leukemia Harboring t(11;14) and 1q Amplification.
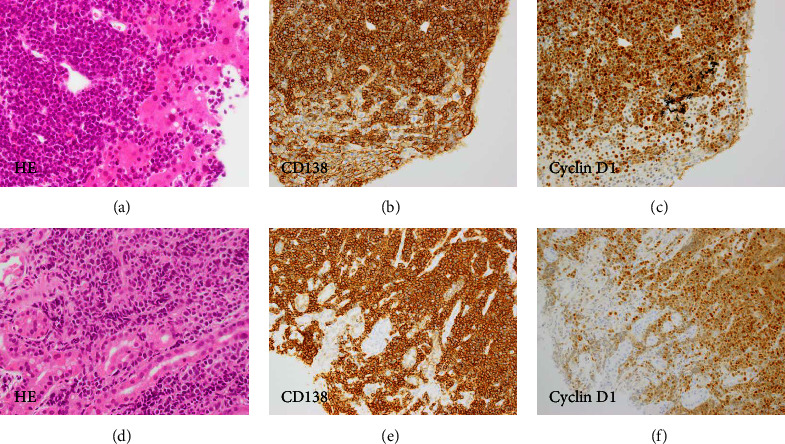
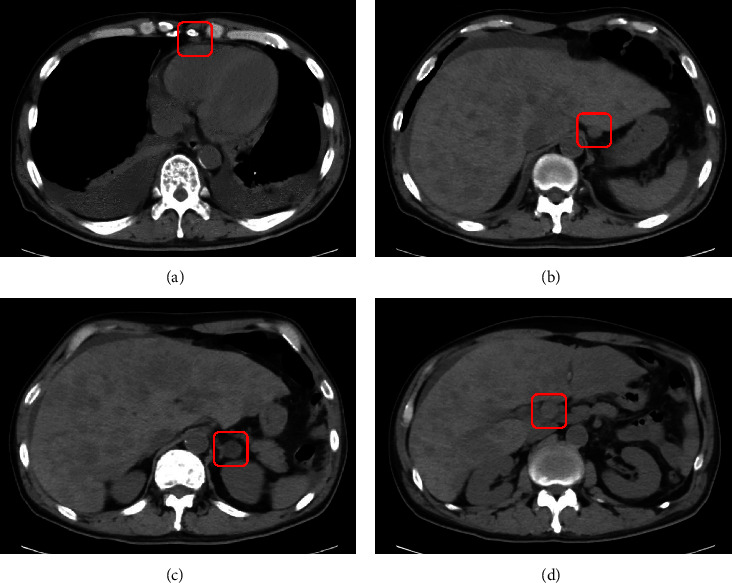
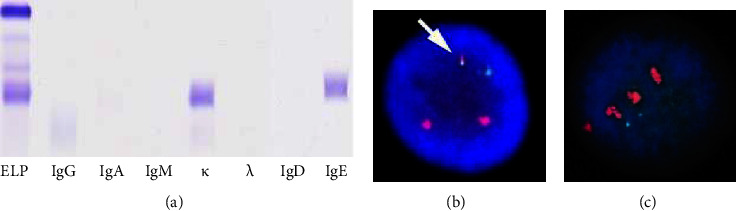
IgE plasma cell neoplasm is the rarest subtype of plasma cell neoplasms and is known for its poor prognosis and high incidence of t(11;14). However, t(11;14) has been classified as a standard-risk rather than high-risk cytogenetic abnormality in multiple myeloma. We have been unable to explain the discrepancy that the hallmark of IgE plasma cell neoplasm with a poor prognosis is a standard-risk cytogenetic abnormality. Here, we report a case of IgE primary plasma cell leukemia with extramedullary lesions of the liver, stomach, and lymph nodes. Plasma cell infiltration was pathologically confirmed in each organ. Cytogenetic analysis of plasma cells revealed t(11;14) and amplification of 1q21. Chemotherapy, with immunomodulatory imide drugs, proteasome inhibitors, and CD38 antibodies, was unsuccessful. In IgE plasma cell neoplasm, coexistence of other cytogenetic abnormalities with t(11;14) may be important. Investigating the presence of cytogenetic abnormalities coexisting with t(11;14) is not only useful for evaluating prognosis but also important for understanding the pathogenesis of the disease. Recently, venetoclax, an oral BCL2 inhibitor, has demonstrated promising efficacy in plasma cell neoplasm patients harboring t(11;14). Development of an effective venetoclax-based regimen for treating aggressive IgE plasma cell neoplasm with t(11;14) is expected.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


