{"title":"肺恶病质对住院患者预后的影响:一项全国性研究。","authors":"Mohamad Alhoda Mohamad Alahmad, Cheryl A Gibson","doi":"10.4103/atm.atm_31_23","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cachexia has been associated with chronic lung disease (pulmonary cachexia syndrome), which is associated with increased mortality. However, studies that looked into this association was relatively small, and national level data are lacking. Herein, we aim to study the association between chronic obstructive lung disease (COPD) and cachexia.</p><p><strong>Research question: </strong>Do patients with COPD and cachexia has worse inpatient outcomes in comparison to those with no cachexia?</p><p><strong>Study design and methods: </strong>We used the Nationwide Readmissions Database from 2016 to 2019, extracting adult patients with a primary diagnosis of COPD who were admitted between January and November of each year studied. We excluded patients with missing data on event time or length of stay. Furthermore, we excluded all cases with cormobidities associated with cachexia. We used SAS 9.4 for data exploration and analysis.</p><p><strong>Results: </strong>We included 1,446,431 COPD-related weighted hospitalizations for which 115,276 cases (7.9%) had a concurrent diagnosis of cachexia (or cachexia-related diagnoses). Overall, patients with cachexia (COPD-C), compared to patients with COPD and no cachexia (COPD-NC), were older (mean age 69 vs. 66 years, respectively, <i>P</i> < 0.001) with similar gender distribution (58%). COPD-C patients had more inpatient complications including cardiac arrest, and use of mechanical ventilation (<i>P</i> < 0.001). Furthermore, they had longer mean lengths of stay (5.2 days vs. 3.8 days, <i>P</i> < 0.001). In-hospital mortality during index, admission was significantly higher in these patients at 2.2% compared to 0.5% for COPD-NC (<i>P</i> < 0.001).</p><p><strong>Conclusion: </strong>COPD-related cachexia is associated with increased inpatient mortality, resource utilization, and prolonged hospitalization.</p>","PeriodicalId":50760,"journal":{"name":"Annals of Thoracic Medicine","volume":"18 3","pages":"156-161"},"PeriodicalIF":2.1000,"publicationDate":"2023-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/4f/f1/ATM-18-156.PMC10473060.pdf","citationCount":"1","resultStr":"{\"title\":\"The impact of pulmonary cachexia on inpatient outcomes: A national study.\",\"authors\":\"Mohamad Alhoda Mohamad Alahmad, Cheryl A Gibson\",\"doi\":\"10.4103/atm.atm_31_23\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Cachexia has been associated with chronic lung disease (pulmonary cachexia syndrome), which is associated with increased mortality. However, studies that looked into this association was relatively small, and national level data are lacking. Herein, we aim to study the association between chronic obstructive lung disease (COPD) and cachexia.</p><p><strong>Research question: </strong>Do patients with COPD and cachexia has worse inpatient outcomes in comparison to those with no cachexia?</p><p><strong>Study design and methods: </strong>We used the Nationwide Readmissions Database from 2016 to 2019, extracting adult patients with a primary diagnosis of COPD who were admitted between January and November of each year studied. We excluded patients with missing data on event time or length of stay. Furthermore, we excluded all cases with cormobidities associated with cachexia. We used SAS 9.4 for data exploration and analysis.</p><p><strong>Results: </strong>We included 1,446,431 COPD-related weighted hospitalizations for which 115,276 cases (7.9%) had a concurrent diagnosis of cachexia (or cachexia-related diagnoses). Overall, patients with cachexia (COPD-C), compared to patients with COPD and no cachexia (COPD-NC), were older (mean age 69 vs. 66 years, respectively, <i>P</i> < 0.001) with similar gender distribution (58%). COPD-C patients had more inpatient complications including cardiac arrest, and use of mechanical ventilation (<i>P</i> < 0.001). Furthermore, they had longer mean lengths of stay (5.2 days vs. 3.8 days, <i>P</i> < 0.001). In-hospital mortality during index, admission was significantly higher in these patients at 2.2% compared to 0.5% for COPD-NC (<i>P</i> < 0.001).</p><p><strong>Conclusion: </strong>COPD-related cachexia is associated with increased inpatient mortality, resource utilization, and prolonged hospitalization.</p>\",\"PeriodicalId\":50760,\"journal\":{\"name\":\"Annals of Thoracic Medicine\",\"volume\":\"18 3\",\"pages\":\"156-161\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2023-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/4f/f1/ATM-18-156.PMC10473060.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Thoracic Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.4103/atm.atm_31_23\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/7/19 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Thoracic Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4103/atm.atm_31_23","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/7/19 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
The impact of pulmonary cachexia on inpatient outcomes: A national study.
Background: Cachexia has been associated with chronic lung disease (pulmonary cachexia syndrome), which is associated with increased mortality. However, studies that looked into this association was relatively small, and national level data are lacking. Herein, we aim to study the association between chronic obstructive lung disease (COPD) and cachexia.
Research question: Do patients with COPD and cachexia has worse inpatient outcomes in comparison to those with no cachexia?
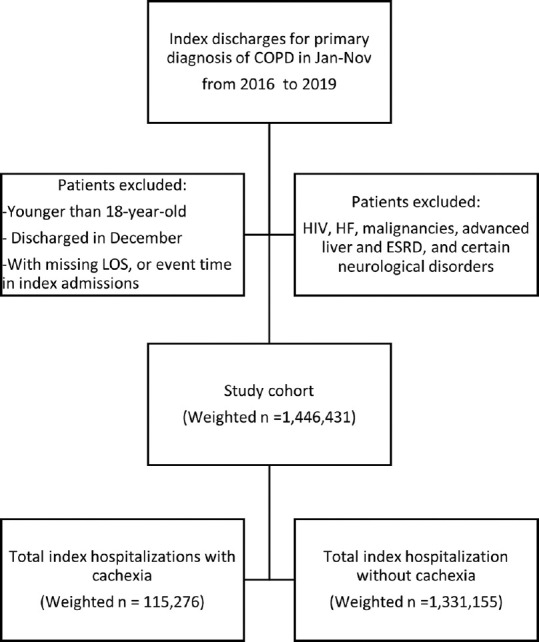
Study design and methods: We used the Nationwide Readmissions Database from 2016 to 2019, extracting adult patients with a primary diagnosis of COPD who were admitted between January and November of each year studied. We excluded patients with missing data on event time or length of stay. Furthermore, we excluded all cases with cormobidities associated with cachexia. We used SAS 9.4 for data exploration and analysis.
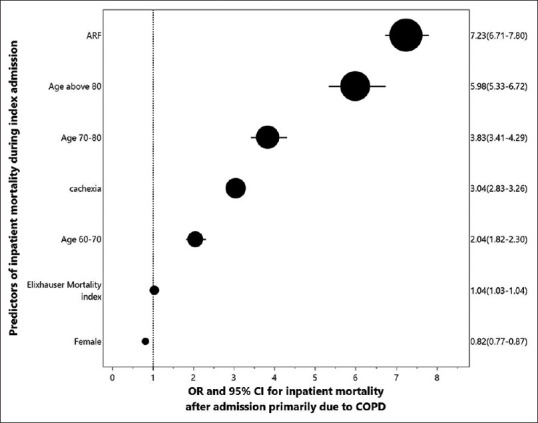
Results: We included 1,446,431 COPD-related weighted hospitalizations for which 115,276 cases (7.9%) had a concurrent diagnosis of cachexia (or cachexia-related diagnoses). Overall, patients with cachexia (COPD-C), compared to patients with COPD and no cachexia (COPD-NC), were older (mean age 69 vs. 66 years, respectively, P < 0.001) with similar gender distribution (58%). COPD-C patients had more inpatient complications including cardiac arrest, and use of mechanical ventilation (P < 0.001). Furthermore, they had longer mean lengths of stay (5.2 days vs. 3.8 days, P < 0.001). In-hospital mortality during index, admission was significantly higher in these patients at 2.2% compared to 0.5% for COPD-NC (P < 0.001).
Conclusion: COPD-related cachexia is associated with increased inpatient mortality, resource utilization, and prolonged hospitalization.
期刊介绍:
The journal will cover studies related to multidisciplinary specialties of chest medicine, such as adult and pediatrics pulmonology, thoracic surgery, critical care medicine, respiratory care, transplantation, sleep medicine, related basic medical sciences, and more. The journal also features basic science, special reports, case reports, board review , and more. Editorials and communications to the editor that explore controversial issues and encourage further discussion by physicians dealing with chest medicine.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


