Elisabeth Greenberg, Elle Schultz, Emily Cobb, Shelia Philpott, Megan Schrader, Jessi Parker
{"title":"社区急诊室胸痛处理中的种族差异。","authors":"Elisabeth Greenberg, Elle Schultz, Emily Cobb, Shelia Philpott, Megan Schrader, Jessi Parker","doi":"10.51894/001c.32582","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Chest pain is one of the most common chief presenting complaints occurring in most Emergency Departments. The HEART score is a validated risk stratification tool commonly used to evaluate chest pain. Prior research has demonstrated the existence of complex racial variations in health care, specifically in what tests are ordered (or accepted by patients) during evaluation and treatment of cardiac disease. The authors hypothesized that chest pain management (i.e., disposition to hospital/observation unit and rates of stress testing) patterns and longitudinal outcomes (i.e., death and 30-day readmission) would occur differently in African Americans despite systematic use of the HEART score.</p><p><strong>Methods: </strong>Funded by the Statewide Campus System, this study was comprised of a retrospective chart review of a sample of eligible patients presenting with chest pain to the authors' 345-bed community-based Michigan hospital.</p><p><strong>Results: </strong>Of the 1,412 eligible sample patients, 886 (63%) reported their racial affiliation as White, 473 (33%) African-American, and 53 (4%) \"Other\". The average HEART score in Whites was 3.92 (SD = 1.89) compared to 3.31 (SD = 1.79) in African-Americans, (p < 0.01, 95% CI: 0.40-0.82). However, White patients' odds of admission to observation or inpatient was 1.49 times higher (95% CI: 1.04 - 2.15), with every unit increase in HEART score increasing the odds ratio of admission by 3.24 times (95% CI: 2.79 - 3.76). White patients were also 2.37 times more likely to receive (or accept) stress tests than African American patients (95% CI: 1.41 - 3.88). Only five (0.01%) of 458 White patients with HEART score between 4 and 6 experienced 30-day readmission or death whereas seven (0.04%) of 193 African-American patients experienced these outcomes (p = 0.04 with OR 3.40, 95% CI: 1.07 - 10.9).</p><p><strong>Conclusions: </strong>Although the authors were unable to precisely distinguish the provider (e.g., desire to order testing) and patient-driven (e.g., desire to accept testing) factors likely to contribute to measured differences, these results suggest continued complex racial variations concerning hospital admission and stress testing in chest pain patients. Further studies are needed to analyze potential systems or subject-level factors influencing the multi-dimensional phenomenon of chest pain management across racial affiliation.</p>","PeriodicalId":74853,"journal":{"name":"Spartan medical research journal","volume":"7 1","pages":"32582"},"PeriodicalIF":0.0000,"publicationDate":"2022-02-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8873438/pdf/","citationCount":"0","resultStr":"{\"title\":\"Racial Variations in Emergency Department Management of Chest Pain in a Community-based Setting.\",\"authors\":\"Elisabeth Greenberg, Elle Schultz, Emily Cobb, Shelia Philpott, Megan Schrader, Jessi Parker\",\"doi\":\"10.51894/001c.32582\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Chest pain is one of the most common chief presenting complaints occurring in most Emergency Departments. The HEART score is a validated risk stratification tool commonly used to evaluate chest pain. Prior research has demonstrated the existence of complex racial variations in health care, specifically in what tests are ordered (or accepted by patients) during evaluation and treatment of cardiac disease. The authors hypothesized that chest pain management (i.e., disposition to hospital/observation unit and rates of stress testing) patterns and longitudinal outcomes (i.e., death and 30-day readmission) would occur differently in African Americans despite systematic use of the HEART score.</p><p><strong>Methods: </strong>Funded by the Statewide Campus System, this study was comprised of a retrospective chart review of a sample of eligible patients presenting with chest pain to the authors' 345-bed community-based Michigan hospital.</p><p><strong>Results: </strong>Of the 1,412 eligible sample patients, 886 (63%) reported their racial affiliation as White, 473 (33%) African-American, and 53 (4%) \\\"Other\\\". The average HEART score in Whites was 3.92 (SD = 1.89) compared to 3.31 (SD = 1.79) in African-Americans, (p < 0.01, 95% CI: 0.40-0.82). However, White patients' odds of admission to observation or inpatient was 1.49 times higher (95% CI: 1.04 - 2.15), with every unit increase in HEART score increasing the odds ratio of admission by 3.24 times (95% CI: 2.79 - 3.76). White patients were also 2.37 times more likely to receive (or accept) stress tests than African American patients (95% CI: 1.41 - 3.88). Only five (0.01%) of 458 White patients with HEART score between 4 and 6 experienced 30-day readmission or death whereas seven (0.04%) of 193 African-American patients experienced these outcomes (p = 0.04 with OR 3.40, 95% CI: 1.07 - 10.9).</p><p><strong>Conclusions: </strong>Although the authors were unable to precisely distinguish the provider (e.g., desire to order testing) and patient-driven (e.g., desire to accept testing) factors likely to contribute to measured differences, these results suggest continued complex racial variations concerning hospital admission and stress testing in chest pain patients. Further studies are needed to analyze potential systems or subject-level factors influencing the multi-dimensional phenomenon of chest pain management across racial affiliation.</p>\",\"PeriodicalId\":74853,\"journal\":{\"name\":\"Spartan medical research journal\",\"volume\":\"7 1\",\"pages\":\"32582\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-02-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8873438/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Spartan medical research journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.51894/001c.32582\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Spartan medical research journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.51894/001c.32582","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Racial Variations in Emergency Department Management of Chest Pain in a Community-based Setting.
Introduction: Chest pain is one of the most common chief presenting complaints occurring in most Emergency Departments. The HEART score is a validated risk stratification tool commonly used to evaluate chest pain. Prior research has demonstrated the existence of complex racial variations in health care, specifically in what tests are ordered (or accepted by patients) during evaluation and treatment of cardiac disease. The authors hypothesized that chest pain management (i.e., disposition to hospital/observation unit and rates of stress testing) patterns and longitudinal outcomes (i.e., death and 30-day readmission) would occur differently in African Americans despite systematic use of the HEART score.
Methods: Funded by the Statewide Campus System, this study was comprised of a retrospective chart review of a sample of eligible patients presenting with chest pain to the authors' 345-bed community-based Michigan hospital.
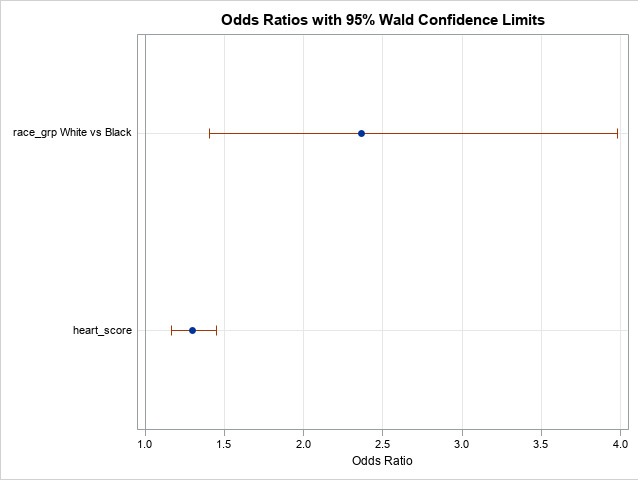
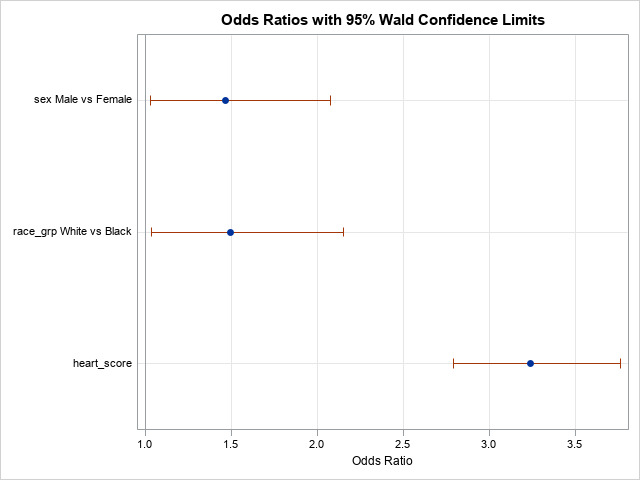
Results: Of the 1,412 eligible sample patients, 886 (63%) reported their racial affiliation as White, 473 (33%) African-American, and 53 (4%) "Other". The average HEART score in Whites was 3.92 (SD = 1.89) compared to 3.31 (SD = 1.79) in African-Americans, (p < 0.01, 95% CI: 0.40-0.82). However, White patients' odds of admission to observation or inpatient was 1.49 times higher (95% CI: 1.04 - 2.15), with every unit increase in HEART score increasing the odds ratio of admission by 3.24 times (95% CI: 2.79 - 3.76). White patients were also 2.37 times more likely to receive (or accept) stress tests than African American patients (95% CI: 1.41 - 3.88). Only five (0.01%) of 458 White patients with HEART score between 4 and 6 experienced 30-day readmission or death whereas seven (0.04%) of 193 African-American patients experienced these outcomes (p = 0.04 with OR 3.40, 95% CI: 1.07 - 10.9).
Conclusions: Although the authors were unable to precisely distinguish the provider (e.g., desire to order testing) and patient-driven (e.g., desire to accept testing) factors likely to contribute to measured differences, these results suggest continued complex racial variations concerning hospital admission and stress testing in chest pain patients. Further studies are needed to analyze potential systems or subject-level factors influencing the multi-dimensional phenomenon of chest pain management across racial affiliation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


